These waves, according to a from Millennium Health, began with the crisis in prescription opioid use, followed by a significant jump in heroin use, then an increase in the use of synthetic opioids like fentanyl.
The latest wave involves using multiple substances at the same time, combining fentanyl mainly with either methamphetamine or cocaine, the report found. “And I’ve yet to see a peak,” said one of the co-authors, , vice president of clinical affairs at , a specialty laboratory that provides drug testing services to monitor use of prescription medications and illicit drugs.
The report, which takes a deep dive into the nation’s drug trends and breaks usage patterns down by region, is based on 4.1 million urine samples collected from January 2013 to December 2023 from people receiving some kind of drug addiction care.
Its findings offer staggering statistics and insights. Its major finding: how common polysubstance use has become. According to the report, an overwhelming majority of fentanyl-positive urine samples ŌĆö nearly 93% ŌĆö contained additional substances. “And that is huge,” said , director of the National Institute on Drug Abuse at the National Institutes of Health.
The most concerning, she and other addiction experts said, is the dramatic increase in the combination of meth and fentanyl use. Methamphetamine, a often in powder form that poses several serious cardiovascular and psychiatric risks, was found in 60% of fentanyl-positive tests last year. That is an 875% increase since 2015.
“I never, ever would have thought this,” Volkow said.
Among the report’s other key findings:
- The nationwide spike in methamphetamine use alongside fentanyl marks a change in drug use patterns.
- Polydrug use trends complicate overdose treatments. For instance, though naloxone, , is widely available, there isn’t an FDA-approved medication for stimulant overdose.
- Both heroin and prescribed opioid use alongside fentanyl have dipped. Heroin detected in fentanyl-positive tests dropped by 75% since peaking in 2016. Prescription opioids were found at historic low rates in fentanyl-positive tests in 2023, down 89% since 2013.
But , an addiction medicine specialist and assistant professor at the University of Colorado’s School of Medicine, warned these declines shouldn’t be interpreted as a silver lining.
A lower level of heroin use “just says that fentanyl is everywhere,” Pytell said, “and that we have officially been pushed by our drug supply to the most dangerous opioids that we have available right now.”
“Whenever a drug network is destabilizing and the product changes, it puts the people who use the drugs at the greatest risk,” he said. “That same bag or pill that they have been buying for the last several months now is coming from a different place, a different supplier, and is possibly a different potency.”
In the illicit drug industry, suppliers are the controllers. It may not be that people are seeking out methamphetamine and fentanyl but rather that they’re what drug suppliers have found to be the easiest and most lucrative product to sell.
“I think drug cartels are kind of realizing that it’s a lot easier to have a 500-square-foot lab than it is to have 500 acres of whatever it takes to grow cocaine,” Pytell said.
Dawson said the report’s drug use data, unlike that of some other studies, is based on sample analysis with a quick turnaround ŌĆö a day or two.
Sometimes researchers face a months-long wait to receive death reports from coroners. Under those circumstances, you are often “staring at today but relying on data sources that are a year or more in the past,” said Dawson.
Self-reported surveys of drug users, another method often used to track drug use, also have long lag times and “often miss people who are active for substance use disorders,” said Jonathan Caulkins, a professor at Carnegie Mellon University’s Heinz College. Urine tests “are based on a biology standard” and are good at detecting when someone has been using two or more drugs, he said.
But using data from urine samples also comes with limitations.
For starters, the tests don’t reveal users’ intent.
“You don’t know whether or not there was one bag of powder that had both fentanyl and meth in it, or whether there were two bags of powder, one with fentanyl in it and one with meth and they took both,” Caulkins said. It can also be unclear, he said, if people intentionally combined the two drugs for an extra high or if they thought they were using only one, not knowing it contained the other.
Volkow said she is interested in learning more about the demographics of polysubstance drug users. “Is this pattern the same for men and women, and is this pattern the same for middle-age or younger people? Because again, having a better understanding of the characteristics allows you to tailor and personalize interventions.”
All the while, the nation’s crisis continues. According to the Centers for Disease Control and Prevention, more than in the U.S. in 2021 from drug overdoses, most because of fentanyl.
Caulkins said he’s hesitant to view drug use patterns as waves because that would imply people are transitioning from one to the next.
“Are we looking at people whose first substance use disorder was an opioid use disorder, who have now gotten to the point where they’re polydrug users?” he said. Or, are people now starting substance use disorders with methamphetamine and fentanyl, he asked.
One point was clear, Dawson said: “We’re just losing too many lives.”
čŅ╣¾Õ·┤½├ĮęĢŅl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFFŌĆöan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-industry/fourth-wave-opioid-epidemic-fentanyl-millennium-health-report/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1816204&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>{kind=link}
The point of contention: For decades, Medicare has paid hospitals ŌĆö including hospital-owned physician practices that may not be physically located in a hospital building ŌĆö about double the rates it pays other doctors and facilities for the same services, such as mammograms, colonoscopies, and blood tests.
The rationale has been that hospitals have higher fixed costs, such as 24/7 emergency rooms and uncompensated care for uninsured people.
Insurers, doctors, and have long complained it’s an unequal and unfair arrangement that results in higher costs for patients and taxpayers. It’s also a profit incentive for hospitals to buy up physician practices, which health economists say can lead to hospital consolidation and higher prices.
In December, the that included a provision requiring Medicare to pay the same rates for , like chemotherapy and many treatments for autoimmune conditions, regardless of whether they’re done in a doctor’s office or clinic owned by a hospital or by a different entity. The policy, known as site-neutral payment, has sparked a ferocious lobbying battle in the Senate, not the first of its kind, with hospitals determined to kill such legislation.
Don’t bet against them. The House legislation would save Medicare an estimated over a decade, according to the Congressional Budget Office. To put this in perspective, the program is projected to pay hospitals upward of $2 trillion during that same period. But hospitals have long argued that any adoption of site-neutral payments would force them to cut jobs or services, or close facilities altogether ŌĆö particularly in rural areas. And senators are listening.
“The Senate is very much attuned to rural concerns,” , who chairs the Finance Committee, told čŅ╣¾Õ·┤½├ĮęĢŅl Health News. His panel has jurisdiction over Medicare, the health program for seniors and people with disabilities.
“I have heard lots of questions about how these proposals would affect rural communities and rural facilities,” he said. “So we’re taking a look at it.”
Outpatient departments at rural hospitals can have outsize importance to their communities. Taking any funding away from stand-alone rural hospitals is seen as risky. in the past decade due to financial problems. With fewer patients, rural hospitals often struggle to attract doctors and update technology amid rising costs.
, a physician who also serves on the Finance Committee, indicated he was apprehensive about the legislation.
“In some cases,” he said, higher Medicare payments for hospitals are “justified.”
“In some cases, it doesn’t seem to be,” he said. He told čŅ╣¾Õ·┤½├ĮęĢŅl Health News he was planning to introduce legislation on the issue but didn’t provide details, and his office didn’t respond to inquiries.
As the two senators show, the issue doesn’t break cleanly along partisan lines. In December, the House easily passed the , the broader bill that included this Medicare payment change, with 166 Republicans and 154 Democrats voting in favor.
“It’s more about how close different members are to the hospital industry,” said , a former White House health economist under President Barack Obama and now a senior fellow at the Brookings Institution.
The American Hospital Association describes the site-neutral policy as a “cut” to hospital Medicare payments and said to a House subcommittee that it “disregards important differences in patient safety and quality standards required in these facilities.”
Chip Kahn, president and CEO of the Federation of American Hospitals, which represents for-profit hospitals, offered a similar characterization of the House-passed legislation. “This is no time for so-called ŌĆśsite neutral’ Medicare cuts that could harm beneficiaries,” he said . He urged lawmakers to drop the policy from the broader bill and instead prioritize access to hospital care for patients by not only protecting Medicare, but also strengthening the health care safety net.
Hospitals argue they need the extra money because they have higher costs, said , an assistant professor of health policy and management at George Washington University and a nonresident fellow at KFF. But “it doesn’t necessarily warrant the amount that they end up getting paid for this,” she said.
The Medicare Payment Advisory Commission, which advises Congress on the program, has recommended implementing site-neutral payments for over a decade.
“This is not a hospital cut. It is rolling back an unethical price increase,” said , a who’s now an executive vice president at founded by John and Laura Arnold, an energy industry investor and an attorney, respectively.
Large hospital systems with the money to buy physician practices, Miller said, have exploited the disparity between Medicare payments to physician offices and hospitals to increase their revenue and consolidate.
Arnold Ventures advocates for site-neutral payments and its leaders have discussed the issue with lawmakers. (The organization has also provided funding for čŅ╣¾Õ·┤½├ĮęĢŅl Health News.)
Miller said he’s hopeful the site-neutral provision of the House bill will be part of a larger government spending bill that must be to keep the government open. If lawmakers need to offset the bill’s costs, “then it is more likely to get in the funding package,” he said.
Though the House-passed legislation is viewed as an “incremental” change, said Fiedler, it faces a rough path forward. Evening out Medicare payment for physician-administered drugs, hospitals fear, could lead to similar moves for other outpatient services.
“Hospitals have a lot of money at stake and will fight this hard,” he said. “Hospitals feel if they lose here, down the road there will be more substantial steps.”
čŅ╣¾Õ·┤½├ĮęĢŅl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFFŌĆöan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-industry/medicare-site-neutral-payments-hospital-lobby-fight/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1813061&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>An estimated 10,000 to 11,000 counselors work at more than 200 call centers nationwide, fielding calls from people experiencing anxiety, depression, or suicidal thoughts.
A , based on responses from 47 crisis counselors, explored variations in their training and work experiences. The survey “is not large enough to support conclusions” about all 988 staffers, said Dan Fichter, the report’s author and a former program manager for the Substance Abuse and Mental Health Services Administration’s 988 team. Still, the first-of-its-kind survey ŌĆö published by CrisisCrowd, a new noncommercial project focused on raising the voices of 988’s workforce ŌĆö surfaced interesting snapshots.
For instance, counselors who responded noted wide variations in training, from four days or less to two weeks.
“We know that there are significant workforce challenges for 988 including staffing shortages and burnout, like much of the health care industry is experiencing today,” Monica Johnson, director of SAMHSA’s 988 & Behavioral Health Crisis Coordinating Office, wrote in a statement. “Ensuring that 988 crisis counselors are properly trained and supported to do this life-saving work is critical.”
Different training approaches emerged as one of the report’s central themes. Most counselors who responded said they were trained in four weeks or less and didn’t consider it adequate.
“I understand that even with about 120 hours of training, we can’t get through all the nuances that boost confidence,” said one anonymous survey response.
Some counselors said they had received training only in talking to people experiencing suicidal thoughts and not how to deal with other mental health issues, such as anxiety attacks, substance intoxication and withdrawal, and mood disorders. They said they had not been prepared for the wide range of calls of varying levels of intensity they would face.
“There could have been more emphasis on how different each convo would be,” noted one.
Some also suggested that opportunities to listen to 988 calls or sessions that used role-playing exercises to practice handling calls would have been helpful.
The risks of counselors not being properly trained are high, said , a member of the California Governor’s Office of Emergency Services’ 9-8-8 Technical Advisory Board and a psychiatrist at . He said it is concerning that some callers may not “feel that they have the support that they need” when reaching out to 988, and “may not call again in the future.” The situation could possibly “cause more stress rather than support,” he added.
, chief advocacy officer of the , said these differences were not a surprise since 988 brought together a patchwork of local and state efforts to provide a hotline specifically for mental health emergencies. In addition, Fichter said, centers’ different training approaches and time frames may “have to do with funding differences that there are between some centers.”
The survey also found that crisis counselors have different expectations for how long they should stay on the phone with callers.
Some counselors, for instance, said they were expected to end conversations with first-time callers and texters who didn’t have immediate plans of suicide within 15 minutes. Others reported limits of up to an hour.
Wesolowski said this issue stood out to her. “That’s certainly not in the spirit of what 988 stands for because there is no exact time that’s perfect to address a crisis,” she said. “Every crisis is unique; every situation, every health seeker is unique.”
The report also noted that centers have different policies on whether counselors should inform callers with imminent plans of suicide or those who are actively attempting suicide that first responders are being dispatched.
Involuntary intervention is used as a last resort to keep someone safe, but some centers believe that telling a caller that police are on their way may lead them to hang up the call, Fichter said. Other centers allow counselors to be transparent with callers about interventions and help callers prepare for the police.
Efforts to make improvements to the hotline’s operations are underway. For example, Vibrant Emotional Health, the company that administers 988, recently created online, self-paced training courses for crisis counselors, according to , Vibrant Emotional Health’s chief 988 Suicide & Crisis Lifeline officer. These classes, she said, are designed to “assist local centers in delivering training and supporting crisis counselor skill development.” She added that these courses are intended to supplement the training local centers already do.
“The success of 988 hinges on those vital people answering calls, texts, and chats every single day,” Wesolowski said of crisis counselors. “They are the heart of this system, and we have to value them. We have to invest in them and give them what they need to be successful.”
čŅ╣¾Õ·┤½├ĮęĢŅl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFFŌĆöan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-industry/988-hotline-counselors-more-training-survey/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1804279&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>But Shen and her husband, who live in Ontario, California, faced a horrible situation. Without intervention, they were told, their baby daughter’s hearing impairment would prevent her from acquiring age-appropriate language skills and likely leave her with developmental problems affecting her education. Pediatric hearing aids can look like modified earbuds and sometimes come in pink, blue, and other bright colors. The ones Emory needed can cost more than , and she would require a new pair about every three years as her ears grow. But the family’s work-based insurance does not cover those costs.
Shen said she knows all too well what’s at stake for her daughter, who was born in February 2023. “If she had hearing aids, I could start all the speech therapy right now, get her access to most of the sounds. But right now, I can’t do anything. Just waiting.”

The family is not alone in this predicament. California and 17 other states don’t require private insurance plans to cover hearing aids for kids, so many don’t. But about two or three of every 1,000 babies in the U.S. are in one or both ears, according to the National Institute on Deafness and Other Communication Disorders.
“You have to learn to hear before you can learn to speak, and we all speak how we hear,” said , a Los Angeles audiologist who co-chairs the volunteer coalition .
Grassroots action, often led by mothers, helped steer legislatures in 32 states to pass bills that would require private insurance to cover hearing aids for children. Vermont, Virginia, and Washington are the most recent.
The fix, however, is not always an easy one. Bills died at the end of the most recent legislative sessions in New York and Hawaii. And, in California, where only enrolled in commercial plans have coverage for hearing aids and services, Democratic Gov. Gavin Newsom in October that would have required such coverage.
“There’s real disappointment among professionals and our California families,” said Phillips.
Newsom, who, by the end of 2023, faced a projected , explained that the bill would “increase ongoing state General Fund costs” and “set a new precedent by adding requirements that exceed the [state’s] ” under the Affordable Care Act. Adding kids’ hearing aids to the essential benefits package would trigger a provision of the ACA that requires state coffers to offset the additional expense. Newsom was wary that this “could open the state to millions to billions of dollars in new costs” for expanded coverage.
Nationally, there’s pressure to pass such state mandates because health plans often don’t cover hearing aids for kids, . , a pediatric ear, nose, and throat physician at the University of California-San Francisco Benioff Children’s Hospitals, said hearing aids should be covered the way glasses and tooth fillings are.
Efforts on the ground suggest the push has slowly been gaining momentum.
Jocelyn Ross of Columbia, South Carolina, founded in 2010 after her daughter Alyssa was diagnosed with congenital hearing loss when she was just a few months old. Although South Carolina has yet to mandate coverage of hearing aids, the coalition has become a model for other such advocacy groups across the nation. was launched a year later by Kelly Jenkins, an Atlanta mom whose daughter has worn hearing aids since she was 18 months old. Legislation requiring the state’s private insurers to cover kids’ hearing aids . Advocates in Ohio and Michigan are also pushing for legislative relief.
Though progress in various states is coming in fits and starts, Newsom’s veto in progressive California was surprising.
Stephanie Wittels Wachs, who founded , has two children who are hard of hearing. Her organization helped push the 2017 passage of kids’ hearing aid legislation. But when she moved from Houston to California in 2020, she was “completely shocked” to learn no such mandate had been approved there. “California usually leads the way, and we are falling behind some more conservative states that have prioritized pediatric hearing loss,” she said.
Newsom’s veto was especially surprising to many advocates because in 2019 he had created the , or HACCP, which offers supplemental coverage of up to $1,500 for hearing aids for families earning up to 600% of the family poverty threshold. Last year’s legislation would have replaced that program, which has proved so far to not be particularly successful, since it began accepting patients in 2021. Provider participation in HACCP is also low. Meanwhile, it’s estimated that 20,115 California enrollees under age 20 need hearing aids and don’t have coverage for them, according to a 2023 report by the .
“We do a great job of diagnosing these kids, we really do,” said Daniela Carvalho, Emory Shen’s audiologist at Rady Children’s Hospital-San Diego. “About more than 99% of kids that are born here are screened. But how can that be a good thing if we’re not following up at six months and giving them what they need to be able to hear? It makes no sense.”
In November, after nearly 10 months, Emory was enrolled in HACCP. Soon she was given loaners, and then she received her own hearing aids in December.
“We talk to her about everything we are doing,” Joyce Shen said. “We tell her about her highchair and her food and the spoon and bowl. Just anything to help develop her speech.”
čŅ╣¾Õ·┤½├ĮęĢŅl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFFŌĆöan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-care-costs/hearing-aids-children-insurance-coverage/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1793583&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>The of nearly 6,300 patients who have had care in the past three years found that about 55% of Black adults feel they have to be very careful about their appearance to be treated fairly by doctors and other health providers. Nearly half of American Indian, Alaska Native, and Hispanic patients feel similarly, as do about 4 in 10 Asian patients.
By comparison, 29% of white people surveyed said they worried about their appearance before appointments.
“In 2023, the notion that any person must prepare for discrimination is sad on one hand and angering on the other,” , executive director of the National Minority Health Association, wrote in an email. “The stress that this causes, in addition to whatever health issue involved, is crazy.”
Discrimination has long been a concern for both patients and health providers in the U.S., where racial disparities in health outcomes are vast and particularly .
A 30-year-old Hispanic man in Illinois who responded to the KFF survey told researchers he wears clothes to health care appointments with the logo of the university where he works. He noticed, he said, that when health care providers know he is a professor, they listen to him more intently and involve him more in care decisions.
A 44-year-old Asian woman in California told the researchers that her white male doctors ignored her concerns about breathing issues, telling her she “was probably just thinking too hard about breathing.” She was later diagnosed with asthma.
The two respondents were not identified in the study.
The survey offers “a way to actually quantify what those experiences are with racism and discrimination, and the multitude of ways they then impact people’s lives,” said , director of KFF’s racial equity and health policy program.
“For folks who have been following these issues for a long time, the findings are not unexpected,” she said.
Other findings:
- A third of adults reported at least one of several negative experiences with a health care provider in the past three years, such as a professional assuming something about them without asking, or suggesting they were to blame for a health problem.
- Nearly a quarter of Black adults, 19% of Alaska Native and Native American adults, 15% of Hispanic adults, and 11% of Asian adults said they believed they endured negative treatment because of their race or ethnicity.
- Twenty-two percent of Black adults who were pregnant or gave birth in the past 10 years said they were denied pain medication they thought they needed. Just 10% of white adults in similar circumstances reported the same complaint.
When people don’t feel respected or welcomed by their health care providers, they may be discouraged to reach out for medical help or may switch providers more often, Artiga said. Members of minority populations are found to be “experiencing worse health as a result of experiencing unfair treatment in the health care system,” she said.
The survey also found that discrimination outside the health care system had health consequences. People who said they experienced discrimination in their everyday lives were more than twice as likely to report often feeling anxious, lonely, or depressed compared with those who rarely or never faced discrimination.
Black people who self-reported darker skin tones were more likely to have encountered discrimination than those with lighter skin, the survey found.
The survey reveals “how persistent and prevalent experiences with racism and discrimination remain today, in daily life and also in health care, despite, really, the increased calls and focus on addressing racism,” said , KFF’s director of public opinion and survey research.
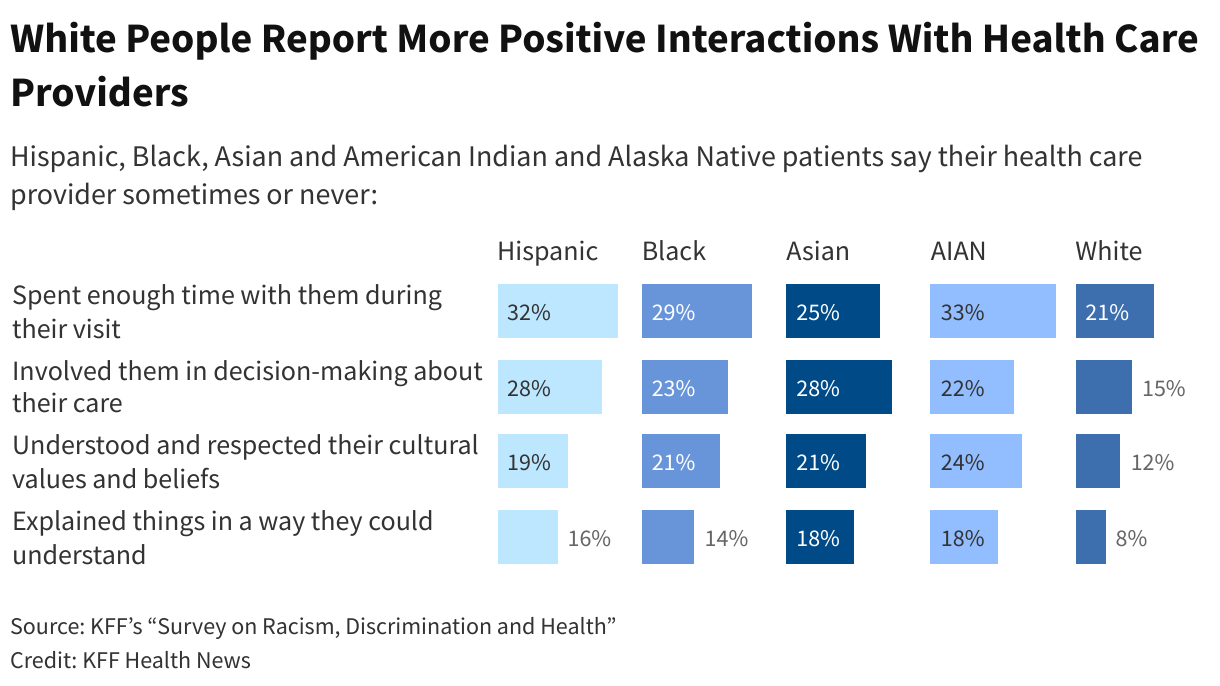
Diversity among health care providers matters, the survey found. Most people of color who participated in the survey said that fewer than half of their medical visits in the past three years were with a provider who shared their race or ethnicity. But Black patients who had at least half their visits with a provider of their race or ethnicity, for example, were more likely to report better experiences, such as their doctor explaining things “in a way they could understand” or asking them about health factors such as their employment, housing, and access to food and transportation.
Nearly 40% of Black adults whose health providers were also Black said they discussed such economic and social subjects, while just 24% of Black adults who saw providers who weren’t Black said those issues were brought up.
Harrison, of the National Minority Health Association, wrote that “a renewed emphasis on recruiting more people of color into the health care field is vital.”
The survey, he added, “painfully illustrates that racial bias in healthcare is as damaging as any disease.”
KFF’s “Survey on Racism, Discrimination and Health” was conducted from June 6 to Aug. 14 online and by telephone among a nationally representative sample of U.S. adults in English, Spanish, Chinese, Korean, and Vietnamese.
čŅ╣¾Õ·┤½├ĮęĢŅl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFFŌĆöan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/race-and-health/health-care-quality-race-appearance-kff-survey/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1781971&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>After introducing the nominee, , at a hearing of the Health, Education, Labor and Pensions Committee, Sanders quickly pivoted to the high prices Americans pay for prescription drugs.
“Let me say a few words about my concerns,” he said, using to detail the failures of the country’s “broken” health system. “Very relevant to the hearing that we are conducting right now,” he said, “we spend, as a nation, the highest prices ŌĆö we pay the highest prices in the world for prescription drugs, in some cases 10 times more than the people in other nations.”
The way the hearing began ŌĆö introducing issues and politics that are not necessarily on point ŌĆö highlights how much the job of leading the NIH has changed. The agency has a budget of more than $47 billion, making it the largest funder of medical research in the world. But the responsibility of its director has, since the pandemic, taken on new layers of complexity.
It has become “an enormous job of bridging between the world of policy, the world of the public, and the world of science,” said Larry Levitt, executive vice president for health policy at KFF.
“Covid turned the scientific health agencies into political footballs like never before,” he said in an interview.
The nomination of Bertagnolli, a surgical oncologist and the director of the NIH’s National Cancer Institute, was applauded by much of the medical research community, especially the oncology world. But after she was tapped for the role in May, progress stalled.
The confirmation of Bertagnolli’s predecessor, , a physician and geneticist, took just four weeks in 2009, Sen. Tommy Tuberville (R-Ala.), observed. Bertagnolli’s, he told her, has “faced a much different nomination process. Your nomination was held up by Chairman Sanders.”
Sanders agreed to hold the hearing only after the Biden administration with for a next-generation monoclonal antibody to prevent covid-19 that required the list price of any resulting drug to be equal to or lower than the price in other major countries.
During the hearing, he returned to the issue, suggesting NIH should seek more such agreements with drugmakers that depend on the agency’s research. He asked Bertagnolli if she could “commit to us that you will work to make sure that Americans do not pay higher prices for prescription drugs in this country than people around the world.”
She responded noncommittally. “It would be a great honor to be able to work with you to make sure that the American people have access to the care that they need to live long and healthy lives.”
As part of his criticism of Sanders, Tuberville also pointed out that the NIH has been without a confirmed director for 21 months. Tuberville, meanwhile, has for months been holding up nominations to military leadership positions over abortion policies.
If she’s confirmed, Bertagnolli would lead the NIH at a time of high scrutiny and skepticism of public health agencies. HELP Committee Ranking Member Bill Cassidy (R-La.) told her that part of her duty would be “to rebuild the relationship with Congress and the public, being a leader that represents the interests of all Americans and not just of the scientific community.”
To this end, senators asked Bertagnolli about how she would lead the agency’s research on maternal health and diabetes, and about how she would address both opioid addiction and mental health crises. She was pressed on how accessible NIH’s data would be to the public.
Roger Marshall (R-Kan.) asked if she thought taxpayers should “fund gender reassignment experiments.” She dodged the question, noting that transgender youth are some of the most vulnerable in the country.
Bertagnolli kept a cool tone throughout the hearing as she shared her vision of “making sure that American people have access and availability and can afford the health care that can save lives.”
Senators also questioned how well-rounded Bertagnolli’s experience is and whether she would favor the NCI over the agency’s 26 other institutes and centers. Sen. Susan Collins (R-Maine) asked Bertagnolli if she would be able to find a balance.
She explained that, as an oncologist, she “took care of patients of all ages, all walks of life, all different health states. I am very familiar to working with colleagues in cardiology, in mental health, in opioid use disorder, in kidney disease, to take care of my patients with cancer.”
The HELP Committee has scheduled a vote on Bertagnolli’s nomination Oct. 25.
čŅ╣¾Õ·┤½├ĮęĢŅl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFFŌĆöan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-care-costs/monica-bertagnolli-nih-nominee-help-committee-sanders/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1762295&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>Then it got busy.
A student fell from the monkey bars and another tripped while playing tag. Two kids hit each other’s heads with lunchboxes and needed ice packs. A young boy had a stomachache. Bobbitt also saw her regular kiddos: one who has special needs and uses a wheelchair and another who has diabetes and gets his blood sugar checked daily before lunch.
“Every day, I’m seeing more and more [youngsters],” Bobbitt, who is a certified nurse practitioner, said with a smile. “I saw more today than yesterday, so we just have to wait and see what the year has in store.”
As the only school nurse at this suburban Washington, D.C., elementary school, Bobbitt’s responsibilities extend beyond treating scraped knees and sniffles for the school’s 600 pupils. At her under-the-sea-themed clinic, she administers medications, teaches kids about health care, and conducts routine health screenings. As the school nurse, she also serves as a public health point person ŌĆö tracking student vaccinations, linking parents to local health care resources, and communicating sometimes difficult messages to them, such as warnings about sexually transmitted diseases and signs of depression.
It’s a full plate, but Bobbitt considers herself lucky. In a previous school nursing job, she split her time between two buildings within the same school district ŌĆö some years three. What hasn’t changed is that school nurses play a critical role in keeping students healthy and ready to learn, but it’s an often-unrecognized field for which schools struggle to attract and retain employees.


More than a third of schools nationwide on-site, according to a 2021 survey by the National Association of School Nurses. The schools that don’t have a dedicated nurse either share one with other campuses, or don’t have one at all. Meanwhile, the nation is facing among K-12 students, such as diabetes and asthma, along with an unprecedented , and ŌĆö often, alone.
School nurses’ roles were further complicated by covid-19. Since the pandemic took hold, they’ve been tasked with tracking cases and tracing exposures. An “extreme load of work was put on school nurses’ shoulders during the pandemic,” said .
They got caught in the middle between anti-maskers and maskers and anti-vaccine and pro-vaccine parents, and were the point of contact whenever students had to quarantine. “School nurses are used to interacting with parents who are angry,” said King, but because of the pandemic “that anger just got to levels we had never seen before.”
In general, kids’ attendance and learning can suffer when students don’t have access to a school nurse. “You’re going to see more absences,” she said, citing a that found students with illnesses or injuries were sent home 18% of the time when evaluated by an unlicensed school employee while only 5% went home after being seen by a school nurse.
Teachers and administrators are shouldering some of the burden by learning how to handle injuries and illnesses themselves, but “it doesn’t take the place of having a school nurse who can respond immediately,” King said.
Though there is no federal law requiring schools to have nurses on staff, the at least one full-time nurse for every 750 students enrolled ŌĆö but most states are missing the mark by miles. School nurses in California have one of the heaviest workloads in the country with a student-to-school-nurse ratio of 2,410 students for every nurse, .
According to research organization , California, along with 34 other states and the District of Columbia, requires schools to employ school nurses. Of those, 12 set required nurse-to-student ratios. Seven states encourage schools to have nurses on staff. Eight states don’t have mandates on the books.
Still, schools were scrambling over the summer to hire nurses.
, a California-based nonprofit organization, said schools struggle not only to retain nurses but also encourage aspiring nurses to consider working in schools. Districts can’t compete with the salaries and benefits hospitals offer. The national median salary for school nurses is , but a registered nurse could make annually working at a hospital.
In some states, school nurses need in addition to their nursing degrees.
The lack of school nurses is a byproduct of a larger issue: the nation’s overall nursing shortage. Health organizations in general ŌĆö even those that offer healthy salaries ŌĆö are facing difficulties hiring and keeping nurses. Around 40% of nurses who participated in a said they were considering leaving their position.
As a nurse for junior high students, King said she is keenly aware that school nurses sometimes serve as students’ only contact with a health care professional, especially at her campus.
World Language Middle School in Columbus, Ohio, where King works, has a diverse student body and takes in many students who are new to the country. “So that requires school nurses like myself to have a very broad range of knowledge of diseases and symptoms,” she said.
Robin Wallin, director of school health services for Alexandria City Public Schools, said that another layer of this issue is that school nursing “is an aging cohort.” The district has at least one school nurse in each of its 18 campuses ŌĆö but this year it was a challenge to fill every spot. That’s partly because many school nurses are aging out, starting to retire, she said. “We need to start to replenish our cohorts.”

Bobbitt said the nursing students who shadow her almost never imagine themselves working in a school. “They want to work in the ER, they want to work in the hospital, they want to work in the NICU, or somewhere where they can have that adrenaline,” Bobbitt said. “This is a little different,” she said, adding that it is fast paced in its own way.
is a clinical coordinator at in New Jersey, and she said one of the biggest learning curves for nurses who opt to work in school settings is that they are “often an independent practitioner,” which involves juggling a lot of responsibilities.
Meanwhile, Bobbitt, working in her brightly colored clinic, stays focused on her daily mission: to address the students’ needs as quickly as possible. “We don’t want them to miss very much school or much class work,” Bobbit said. “That’s our goal, right?”
This <a target="_blank" href="/health-industry/school-nurses-shortage-mental-health/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1752567&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>Hanke remembers the night 13 years ago when Charlie, then 3 weeks old, was fussier than usual, so he picked him up to soothe him back to sleep. With Charlie still in his arms, he sat on the couch, turned on the TV, and nodded off.

“We were kind of chest to chest, the way you see in pictures a lot,” Hanke said. But he didn’t realize Charlie’s airways were blocked. Too young to turn his head, too squished to let out a cry, Charlie died silently. The next morning, Hanke woke up to his worst nightmare. Years of medical school weren’t enough to prevent Hanke from losing Charlie to accidental suffocation.
, a well-known term that describes unexplained but natural infant deaths resulting from an unknown medical abnormality or vulnerability, is the leading cause of unexpected deaths among infants in the U.S. It has long been among new parents’ greatest fears.
Rates for SIDS have declined since the 1990s, but a different cause of infant death ŌĆö accidental suffocation or strangulation ŌĆö has also been a persistent problem. That national rate for the past decade has hovered between 20 and 25 infant deaths per 100,000 live births, accounting for around a fifth of all unexpected infant deaths, according to the . Accidental suffocations and strangulations aren’t necessarily happening more often, some experts say; rather, fatality review teams have become better at identifying causes of death.
And the trend remains steady despite decades of public information campaigns imploring parents to take steps to keep their babies safe while sleeping.
In the mid-1990s, the launched its “Back to Sleep” campaign, to teach parents to lay infants on their backs to sleep. “There were tremendous results after ŌĆśBack to Sleep,’” said , executive director of , a Connecticut-based nonprofit group focused on safe sleep education. Unexpected infant deaths dipped about 40% from 1990 levels, which was before that campaign launched, according to the CDC. “But then it plateaued,” Jacobson said.
The NICHD eventually broadened this message with other ways to limit risks beyond a baby’s sleep position with the “” initiative.
Some clear warnings from it: Infants shouldn’t sleep with blankets, stuffed toys, or bumpers that “can potentially lead to suffocation or strangulation,” said , program coordinator for in Fort Worth, Texas. They also should sleep in cribs or bassinets ŌĆö not on beds with siblings or in parents’ arms.

But these public health messages ŌĆö contradicted by photos or videos circulating in movies and social media ŌĆö don’t always find traction. Professional photos of infants, for example, too commonly show them peacefully snoozing surrounded by plush animals and blankets. St. John added that parents sometimes have preconceived ideas of how infants’ sleeping spaces should be decorated. “When you think of cribs and nurseries and things like that, you imagine the pictures in the magazines,” St. John said. “And those are beautiful pictures, but it doesn’t keep your baby safe.”
St. John said many parents know that babies should be on their backs to sleep, but warnings about strangulation by blankets or suffocation by sharing a bed with them sometimes fall through the cracks.
For instance, new parents, especially single parents, are more likely to accidentally fall asleep with their infants because of exhaustion, said , a neonatologist at Cincinnati Children’s Hospital.
The idea that sleeping with one’s baby is dangerous can also be counterintuitive to a new parent’s instinct. “We feel like being close to them, being able to see them, being able to touch them and feel that they’re breathing is the best way we can protect them and keep them safe,” said Miller, who is also an assistant professor at the University of Cincinnati’s Department of Pediatrics.
Organizations across the country are working to help parents better understand the true risks. Hanke and his wife, for instance, channeled their grief into , a nonprofit focused on safe sleep practices for infants. The Hankes also wrote a book, “,” which has sold about 5 million copies. The proceeds are used to continue their educational efforts.
Ohio, where Charlie’s Kids is based, in 2020 saw 146 , a classification that includes SIDS, accidental suffocation and strangulation, and other instances in which the cause is undetermined. That’s about a death for every 1,000 live births, according to the . Thirty-six percent of those deaths were attributed to accidental suffocation or strangulation. Nationally, the rate of these unexplained deaths has declined since the 1990s, but, according to the CDC, significant racial and ethnic differences continue.
The particular risks for an infant’s accidental suffocation in many respects are situational ŌĆö and often involve people at the lower end of the income scale who tend to live in close quarters. People who live in a small apartment or motel often share sleep space, said St. John.
Tarrant County has one of Texas’ highest rates of infant deaths ŌĆö three to four each month ŌĆö attributed to accidental suffocation.
So, organizations like the , which serves Fort Worth and parts of Dallas, have been providing free bassinets and cribs to those in need.
County representatives spoke during the state’s Child Fatality Review Team meeting in May and focused on the prevalence of infant deaths linked to accidental suffocation. For the past decade, data shows, the county has averaged 1.05 sudden unexpected infant deaths per 1,000 births, which is higher than both the state and national averages of 0.85 and 0.93, respectively. During a 15-month period starting in 2022, Cook Children’s Medical Center saw after they left because of unsafe sleeping environments.
Sometimes parents’ decisions are based on fears that stem from their environments. “Parents will say ŌĆśI’m bringing my baby into bed because I’m afraid of gunshots coming through the window, and this is how I keep my baby safe’ or ŌĆśI’m afraid rats are going to crawl into the crib,’” said First Candle’s Jacobson.
She understands these fears but stresses the broader context of safe sleep.
The key to educating parents is to begin when they are still expecting because they receive “a load of information” in the first 24 or 48 hours after a baby is delivered, said , a neonatal-perinatal specialist at in San Antonio. Garza-Cox is also a member of the Bexar County Child Fatality Review Team.
And once a child is born, the messaging should continue. In Connecticut, for instance, First Candle hosts monthly conversations in neighborhoods that bring together new parents with doulas, lactation consultants, and other caregivers to discuss safe sleep and breastfeeding.
And both Tarrant and Bexar counties are placing ads on buses and at bus stops to reach at-risk parents and other caregivers such as children, relatives, and friends. Parents are very busy, Garza-Cox said. “And sometimes, multiple children and young kids are the ones watching the baby.”
čŅ╣¾Õ·┤½├ĮęĢŅl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFFŌĆöan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/public-health/safe-infant-sleep-sids-suffocation-strangulation-messaging/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1740164&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>The Republican governor signed House Bill 2127 ŌĆö known as the Texas Regulatory Consistency Act but dubbed the “Death Star” by critics ŌĆö the same month the state saw at least amid a scorching heat wave that’s .
The measure, heavily backed by business and building sectors, was designed to replace “the regulatory patchwork” of county and municipal rules across the state “with a single set of predictable, consistent regulations,” according to circulated by its supporters. That means cities would no longer have the authority to enforce local ordinances related to agriculture, natural resources, finance, and labor; and local protections against extreme heat, such as water break requirements, would be rolled back.
The group of about three dozen people stood in the early-afternoon sun and held signs that read “Working Shouldn’t Be a Death Sentence,” “Water Breaks = Basic Right,” and “People Over Profits,” sweating and squinting. In the nation’s capital, the heat index had already reached 91 degrees. But protesters were focused on the plight of employees working in their even-hotter home state, where the thermostat had been reaching triple digits.
(D-Texas), who organized this week’s protest, joined more than 100 other U.S. legislators in urging acting Labor Secretary Julie Su to continue the development and implementation of federal standards for rest and water breaks to prevent occupational heat illness and death.
Casar, along with others in the group, including members of San Juan, Texas-based and civil rights activist , didn’t eat or drink from 10:30 a.m. to 6:30 p.m., both to push for national action to reverse Abbott’s law and as a sign of solidarity with Texas employees, especially those who work outside.
“A basic thing like the right to a water break, a basic thing like being able to go to work and know that working is not a death sentence, is the baseline of what our democracy should be able to do,” Casar said, with sweat dripping from his forehead.
Huerta, 93, who worked alongside the legendary to create organizations like La Unión, reminded the crowd that in the 1960s went on strike to protest poor and dangerous working conditions, including the lack of job security, bathroom access, and water during the day.
“This is such a cruel thing,” Huerta said.


A steady stream of lawmakers came by to express support for the rally, including House Minority Leader Rep. Hakeem Jeffries of New York and well-known progressives like Sen. Bernie Sanders (I-Vt.), Rep. Alexandria Ocasio-Cortez (D-N.Y.), and other members of “The Squad,” a small group of . And from California, , Democratic Reps. Katie Porter, who is running for the Senate, and Ro Khanna also made appearances. California is among those states that have rules in place to protect workers from extreme heat.
was in attendance and challenged Abbott to spend a day without water. “One day in the governor’s mansion, the air-conditioned governor’s mansion, without water,” he said. “Or better yet, one day with the folks who are out in the fields, the folks who are out on top of roofs, the folks who are at construction sites.”
At the front of the crowd were Jasmine and Daisy Granillo, younger sisters of Roendy Granillo, a construction worker of Fort Worth, Texas, who died in July 2015 from heat exhaustion. He was 25 and was installing hardwood flooring in a house without ventilation. The temperature was in the high 90s, he was wearing extra layers of protection because of the chemicals in the wood, and his request for a water break was denied. “My parents were told that his organs were cooked from the inside,” Jasmine said.
On the day Roendy passed away, he told his sisters he would take them to the flea market when he came home from work. He didn’t come home. They’re now committed to making sure others don’t suffer from heat exhaustion as he did. “I know that a simple water break, a simple water break, could have prevented his death,” Jasmine told čŅ╣¾Õ·┤½├ĮęĢŅl Health News.
This is the second time Jasmine and her family have rallied for water breaks for outdoor workers. After her brother died, she and others pushed the Dallas City Council in 2015 to establishing 10-minute rest breaks every four hours for construction workers. In 2010, Austin passed its own such rule. Abbott’s law, set to take effect Sept. 1, will dissolve those ordinances and prohibit local governments from passing similar ones.

The protesters gathered at the Capitol steps also said they worried that corporate interests would try to block the national rule from seeing the light of day. “They delay them as long as they can until they die a slow death, and we’re here today to make sure that doesn’t happen,” Casar said.
Taylor Critendon, a registered nurse who specializes in critical care at in Austin, attended the event to monitor the congressman’s vitals and keep an eye on the group’s well-being. She said she has been treating more patients because of heat exhaustion than before. “It’s definitely taking a toll on our community,” she said.
She emphasized that not drinking enough water while outside in hot temperatures can cause someone’s heart rate to rise and blood pressure to drop. Often, patients start to feel weak and faint and lose blood flow, she said, referencing the body’s internal mechanism to cool itself down. People shouldn’t wait to experience these symptoms before drinking water.
“When you’re thirsty, then you’re already farther down the line of dehydration,” Critendon said, explaining why outside workers need regular water breaks. “You can’t really wait until your body says, ŌĆśOh, I’m thirsty,’ because by that time it’s already late.”
, president and executive director of La Unión del Pueblo Entero, also participated in the daylong hunger and thirst strike. The union has historically protected the rights of migrant farmworkers in South Texas but has more recently expanded to include others, such as construction workers.
“We’ve been here for just about an hour,” she said. “We’re sweating” and “it’s really, really hot,” she added. “Can you imagine what it is like for construction workers every single day?”
This <a target="_blank" href="/public-health/texas-heat-outdoor-workers-water-break-thirst-strike-governor-greg-abbott/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1726073&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>The hotline was designed with the idea that people experiencing emotional distress are more comfortable reaching out for help from trained counselors than from police and other first responders through 911.
Since the federally mandated crisis hotline’s new number launched in July 2022, 988 has received calls, chats, and texts, according to ŌĆö up 33% from the previous year. (The hotline previously used a 10-digit number, 800-273-8255, which remains active but is not promoted.)
At a , policymakers and mental health experts celebrated the hotline’s first-year successes as well as its additional $1 billion in funding from the Biden administration. Health and Human Services Secretary Xavier Becerra described 988 as a “godsend” during taped remarks. “It may not be the solution,” he said, “but it lets you touch someone who can send you on a path to where you will get the help you need.”
Those same advocates recognized the dark reality represented by 988’s high call volume: The nation faces a mental health crisis, and there is still much work to be done.
One year in, it’s also clear that the 988 hotline, a network of more than 200 state and local call centers, faces challenges ahead, including public mistrust and confusion. It’s also clear the hotline needs federal and state funding intervention to be sustainable.
Here’s a status check on where things stand:
What Worked?
The original 1-800 national mental health crisis hotline has operated since 2005. The huge increase in calls to 988 compared with those to the 1-800 number in just a year is likely linked to the simplicity of the three-digit code, said , vice president of policy and communications at Behavioral Health System in Baltimore. “People are remembering it easily,” she told čŅ╣¾Õ·┤½├ĮęĢŅl Health News.
According to a conducted in June, 63% of Americans had heard of 988, and those ages 18 to 29 were most aware. Additionally, the survey found that LGBTQ+ people were twice as likely to be familiar with 988 as people who don’t identify as LGBTQ+.
The 988 hotline provides 24/7 support for people in suicidal crisis or other kinds of emotional distress, Breidenstine said. “They can be calling if they really just had a bad day,” she said. “We also get some calls from people experiencing postpartum depression.” Callers are directed to a menu of options to choose which kind of service would best help them, including a veterans’ line.
As it launched, mental health experts worried about the hotline’s ability to keep up with demand. But it appears to be growing into its position. “Despite a huge increase of demand on the system, it’s been holding up, and it’s been holding up exceptionally well,” , chief advocacy officer at the , told čŅ╣¾Õ·┤½├ĮęĢŅl Health News. It now takes for someone reaching out to 988 ŌĆö by calling or texting ŌĆö to reach a counselor, according to data from the Substance Abuse and Mental Health Services Administration. A year ago, that average was one minute and 20 seconds.
Wesolowski said one of the biggest surprises with the launch was the frequency of text-message traffic. In November 2022, the Federal Communications Commission voted to require 988 to be texting-friendly.
In May, according to SAMHSA, 988 received about 71,000 texts nationwide with a 99% response rate, compared with 8,300 texts in May 2022 with an 82% response rate.
This month, HHS text and chat services to 988.
Challenges Ahead
More than half of Americans have heard of 988, but only a small fraction understand how the hotline operates. According to NAMI’s survey, only 17% of people who responded said they were “very/somewhat familiar” with the hotline.
Most people think that by calling 988, like 911, emergency services will automatically head their way, the survey found. Currently, 988 does not use geolocation, meaning call centers don’t automatically receive information about callers’ locations. , which operates the hotline, is working to incorporate geo-routing into the system, which would help identify callers’ regions ŌĆö but not exact locations ŌĆö making it possible to connect them to local counseling groups and other mental health services.
But incorporating geo-routing into the hotline isn’t without controversy. When it launched, people responded on social media with warnings that calling 988 brought a heightened risk for police involvement and involuntary treatment at psychiatric hospitals. “Based on the trauma that so many people in the mental health community have long experienced when they’ve been in crisis, those assumptions are very understandable,” Wesolowski said.
Fewer than 2% of calls end up involving law enforcement, she said, and most are de-escalated over the phone.
“The vast majority of people think that an in-person response is going to happen whenever you call ŌĆö and that’s just simply not true,” Wesolowski said.
Another challenge mental health advocates face is informing older adults about 988, especially veterans, who are at higher risk of having suicidal ideations. Americans ages 50 to 64 had the lowest awareness rate of 988 ŌĆö at 11% ŌĆö among all age groups, according to NAMI’s survey.
This is a telling sign of how older generations are less willing to discuss and admit to mental health struggles, Wesolowski said. “Young people are just more willing to be open about that, so I think that breaking down that stigma across all age groups is absolutely vital, and we have a lot of work to do in that space.”
Is 988 Sustainable?
Since the hotline launched, it has been dependent on federal grants and annual appropriations. A gush of funding flowed when 988 launched, “but those annual appropriations are something you have to keep going back for year after year, so the sustainability aspect is a little more fraught,” Wesolowski said.
This is where Congress and state legislatures come in.
Mental health leaders hope to push legislation that allows 988 to be funded the same way 911 is nationwide. mandated 911 to be the country’s universal emergency number, and ever since, users have automatically been charged ŌĆö ŌĆö on their monthly phone bills to fund it. Six states have imposed a similar tax for 988, and two states ŌĆö and ŌĆö have bills for this tax on their governor’s desks.
It’s under the FCC’s power to levy a nationwide tax, but the federal agency hasn’t done so yet.
čŅ╣¾Õ·┤½├ĮęĢŅl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFFŌĆöan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-industry/a-year-with-988-what-worked-what-challenges-lie-ahead/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1723706&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>