“Every little ache, like my knee hurts,” she said, made her worry that “this is the end of the road for me.”
So Zapp, a 40-year-old communications director in New York, became one of millions of Americans to start taking an anxiety medication in recent years. For her, it was the serotonin-boosting drug Lexapro.
“I love it. It’s been great,” she said. “It’s really helped me manage.”
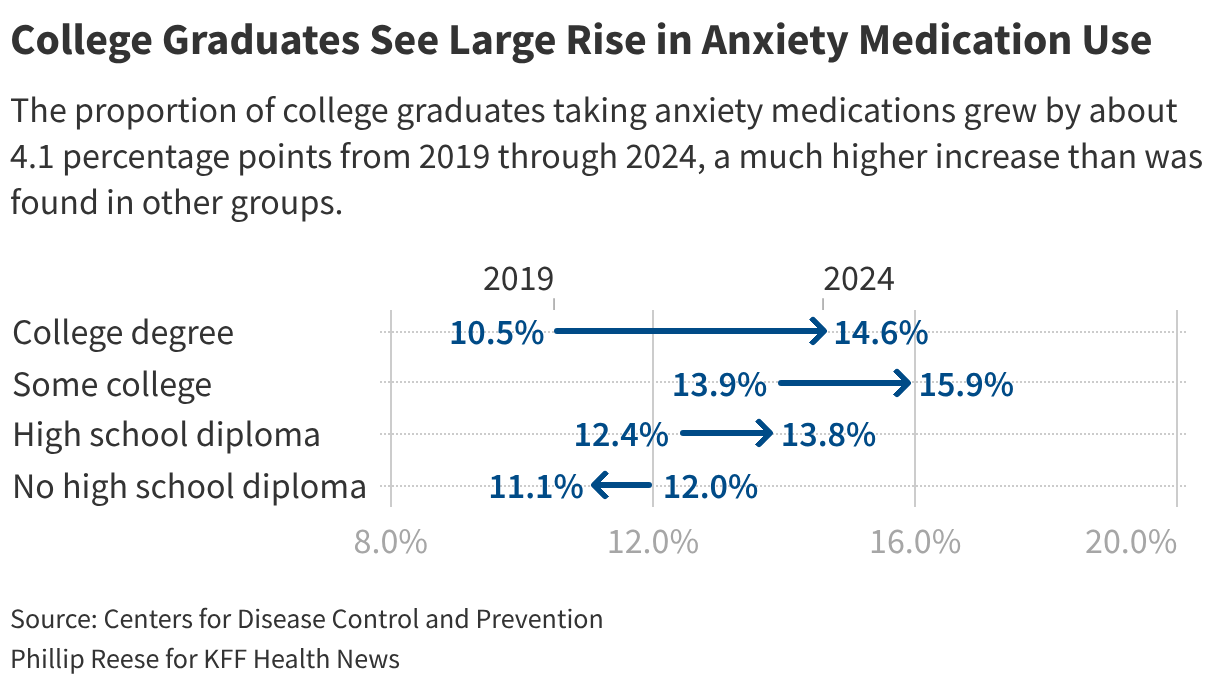
The proportion of American adults who took anxiety medications jumped from 11.7% in 2019 to 14.3% in 2024, with most of the increase occurring during the covid pandemic, according to from the Centers for Disease Control and Prevention. That’s 8 million more people, bringing the total to roughly 38 million, with sharp increases among young adults, people with a college degree, and adults who identify as LGBTQ+.
Even as psychiatric medications gain public acceptance and become easier to access through telehealth appointments, the rise of a class of antidepressants called selective serotonin reuptake inhibitors, known as SSRIs, has triggered a backlash from supporters of the “Make America Healthy Again” movement who argue they are harmful. Doctors and researchers say medications such as Prozac, Zoloft, and Lexapro are front-line treatments for many anxiety disorders, including generalized anxiety disorder and panic disorder, and are being misrepresented as addictive and broadly harmful even though they’ve been proved safe for extended use.
Health and Human Services Secretary Robert F. Kennedy Jr. has decried broadening SSRI use. During his Jan. 29 confirmation hearing, he said he knows people, including family members, who had a than people have quitting heroin. More recently, he a possible link between the use of SSRIs and other psychiatric medications and violent behavior like school shootings.
Food and Drug Administration Commissioner Marty Makary that SSRI use among pregnant women could lead to poor birth outcomes.
SSRIs’ common side effects include . Some SSRIs also and cause other sexual side effects.
For many people, however, the side effects are mild and tolerable and the benefits of treating chronic anxiety are worth it, said , president of the Southern California Psychiatric Society. “The statements about SSRIs were just not grounded in any sort of evidence or fact,” Kelly said of Kennedy’s comments.
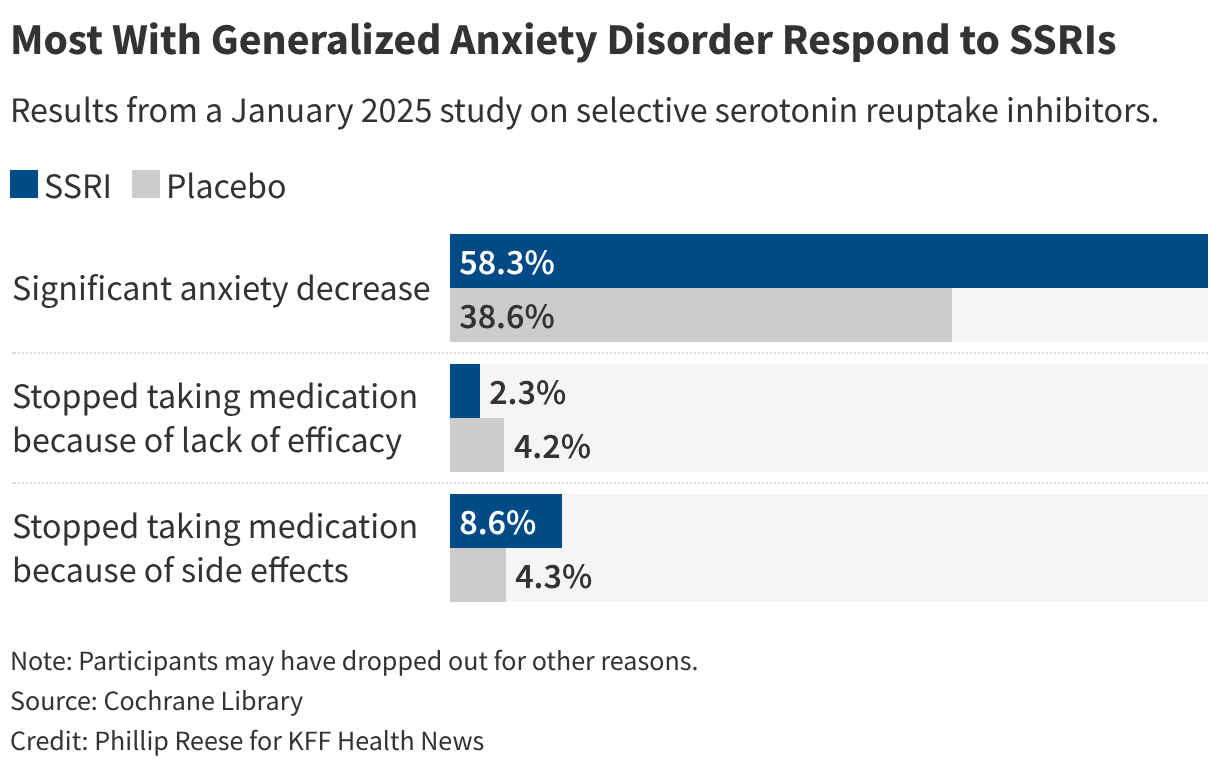
A showed that over half of people with generalized anxiety disorder taking an SSRI saw their anxiety symptoms reduced by at least 50%. Side effects prompted about 1 in 12 to stop taking an SSRI.
“When it’s being done right and when you’re also using appropriate therapy techniques, SSRIs can be really, really helpful,” said , a psychiatrist who practices in Los Angeles.
MAHA Blames Anxiety on Poor Diet, Lack of Exercise
Supporters of MAHA have partly blamed poor dietary choices and the increase of a sedentary lifestyle for the rise of a number of health problems, including anxiety, depression, and other mental health disorders. As a remedy, they have called for measures such as reducing consumption of ultraprocessed foods, which to depression and anxiety, and cutting back on screen time in favor of exercise.
Psychiatrists often encourage a and exercise as an for . Wood said those who can manage anxiety without medication should also consider talk therapy. The proportion of American adults using mental health counseling boomed from 2019 to 2024 as teletherapy grew in popularity, federal data shows. “Anxiety disorders are amongst our psychiatric disorders that really respond well to cognitive behavioral therapy,” she said.
But medication can help.
Studies show the risks of taking SSRIs during pregnancy for mother and child. By contrast, “depression increases your risk for every complication for a mother and a baby,” Wood said, adding that recent statements by government officials about SSRI use during pregnancy are “potentially leading to real harm for these women.”
Some people who stop taking antidepressant medication , especially if they quit suddenly. But “the concept of addiction simply does not apply to these chemicals,” Kelly said, a statement .

Addiction, though, is a possibility with benzodiazepines such as Xanax that are often a second line of treatment for anxiety. These controlled substances can also in patients taking both types of drugs. During congressional hearings last year, Kennedy also decried benzodiazepine overuse as a problem.
While benzodiazepines are effective for short-term use, they require monitoring and care, Wood said.
“Those are really great meds for acute anxiety and not great as long-term anxiety medications, because they are habit-forming over time,” Wood said. “If you’re taking them on a daily basis, you’ll need more and more to get the same effect, and then you have to come down from them in a tapered way.”
And an are also occasionally taking beta-blockers such as propranolol for anxiety. Some people use beta-blockers to prevent a racing heart before a public speech or other big moments, even though they are not FDA-approved for treating anxiety and are prescribed “off-label.”
Beta-blockers , but they are “nonaddictive, really helpful for bringing down the autonomic nervous system, going from fight or flight to something more neutral, and really safe,” Wood said.
Social Shifts Drive Increased Use of Anxiety Meds
A number of could explain why so many more people are taking anxiety medication, increased social media use, more isolation, and heightened economic uncertainty, physicians and researchers say.
Plus, the medicines are relatively easy to get. Many people obtain SSRI and benzodiazepine prescriptions from their primary care physician. Others obtain the medications .
Many social media influencers , easing some stigma among young people and encouraging them to get help. About a third of teens said they get mental health information via social media.
Still, increased access to anxiety medication can be a problem when combined with a trend of self-diagnosis based on social media trends. A Google search for “” leads to sponsored promises of same-day treatment, though fine-print disclaimers clarify that a prescription is not guaranteed.
“I think increased access is good, but that’s not the same thing as, you know, ordering Xanax online,” Kelly said.
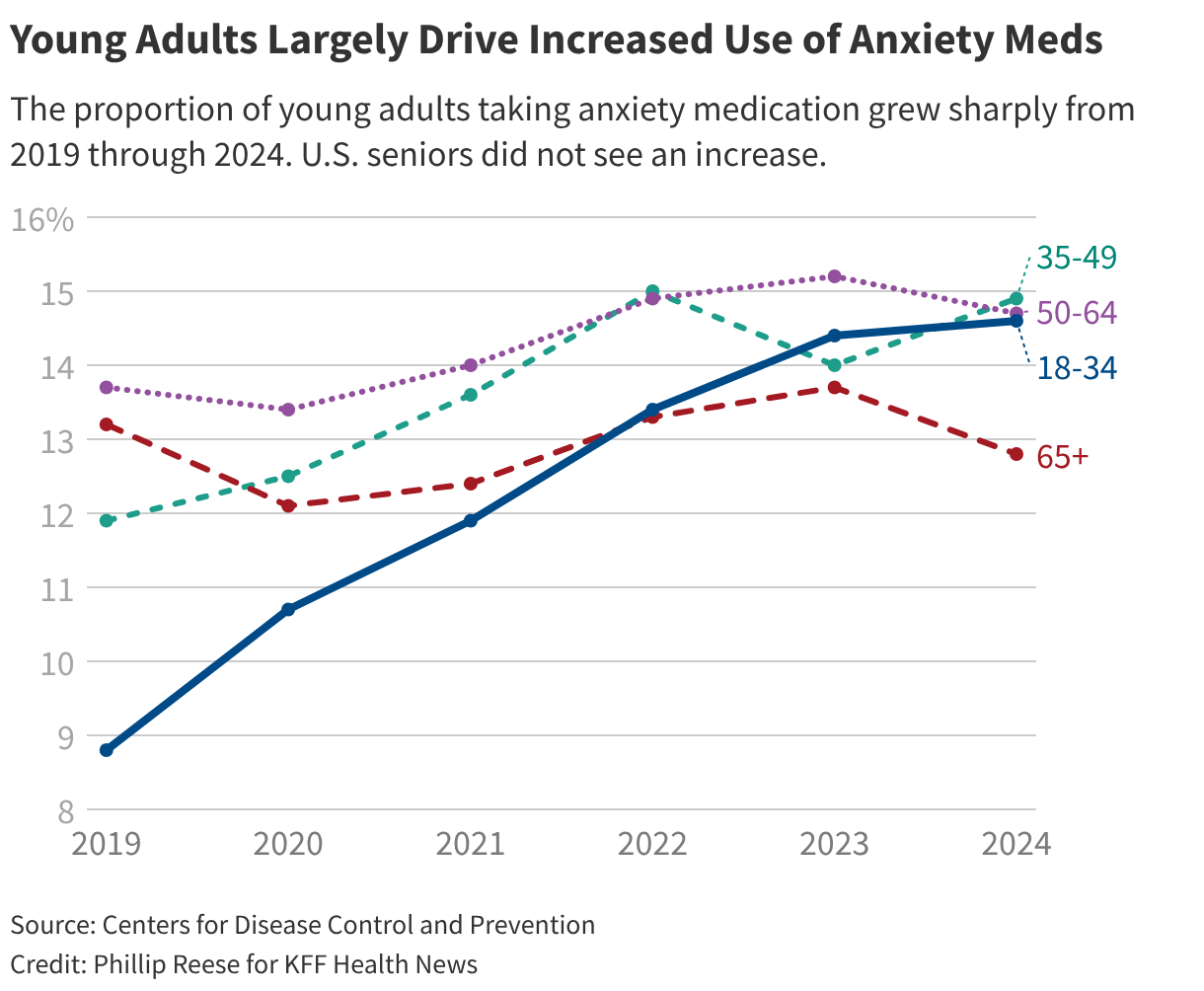
Young adults are largely driving an increase in anxiety medication use. The proportion of Americans ages 18 to 34 taking anxiety medication rose from 8.8% in 2019 — the first year such survey data became available — to 14.6% in 2024. By contrast, the rate didn’t change much among adults 65 and older, CDC data shows.
The pandemic and covid lockdowns greatly increased stress among many American adults, .
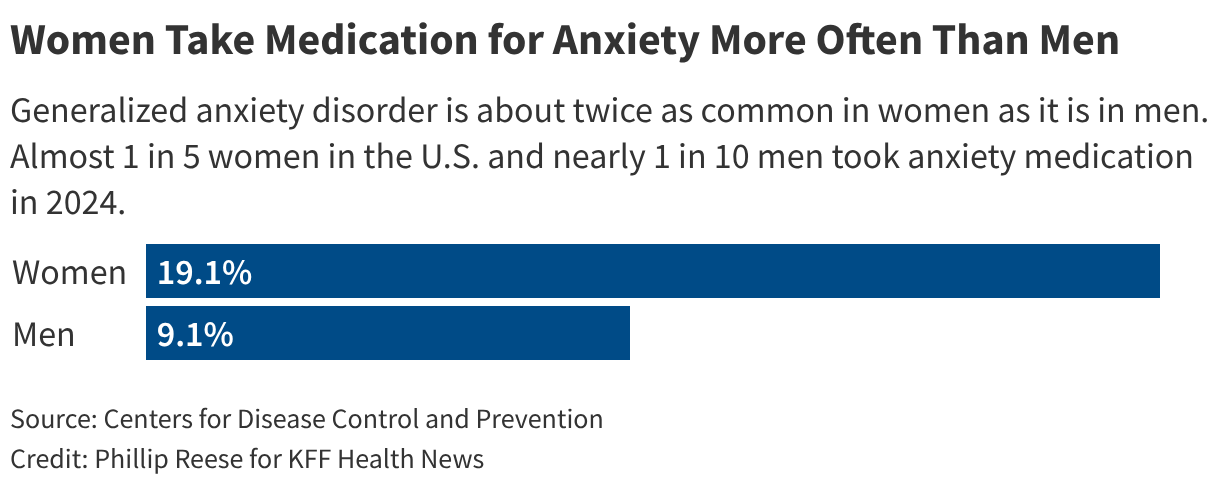
And data shows more women than men take anxiety medication. , a department chair and professor of sociology at the University of Pennsylvania, said that’s because they’re more likely to need them. They are also likelier than men to report when they feel anxious, and doctors are “inclined or see anxiety more readily in their female patients than their male patients,” Schnittker added.
Broader trends could also be at work. Schnittker said studies have shown anxiety growing more prevalent among ensuing generations for much of the 20th and 21st centuries. Schnittker, author of , said growing income inequality could be partly to blame, with people feeling stress over improving their economic status. Social and religious activities have been replaced by more isolation. And people have become more suspicious of others, creating a sense of unease around strangers.
For Zapp, the cancer survivor, it took a few months on Lexapro before she started seeing clear results. When she did, she said, it felt like her mind was less noisy, making it easier to focus. She also underwent talk therapy, but now her chronic anxiety is stabilized on medication alone.
“It definitely helped me get back to my day-to-day in a way that was productive and not just riddled with my anxieties throughout the day,” she said.

Ńîąóĺú´«Ă˝Ň•îl Health News’ Holly Hacker, Maia Rosenfeld, and Lydia Zuraw contributed to this report.
Ńîąóĺú´«Ă˝Ň•îl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-industry/anxiety-medications-ssris-prozac-zoloft-lexapro-maha-kennedy-rfk-jr/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=2155784&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>{kind=link}
Not one U.S. citizen has applied.
West River Health Services in Hettinger, a town of about 1,000 residents in the southwestern part of the state, has four options, and none is good.
The hospital could fork over $100,000 for the Trump administration’s new H-1B visa fee and hire one of the more than 30 applicants from the Philippines or Nigeria. The fee is the equivalent of what some rural hospitals would pay two lab techs in a year, said Holzkamm, who is West River’s lab manager.
West River could ask the Department of Homeland Security to waive the fee. But it’s unclear how long the waiver process would take and if the government would grant one. The hospital could continue trying to recruit someone inside the U.S. for the job. Or, Holzkamm said, it could leave the position unfilled, adding to the workload of the current “skeleton crew.”
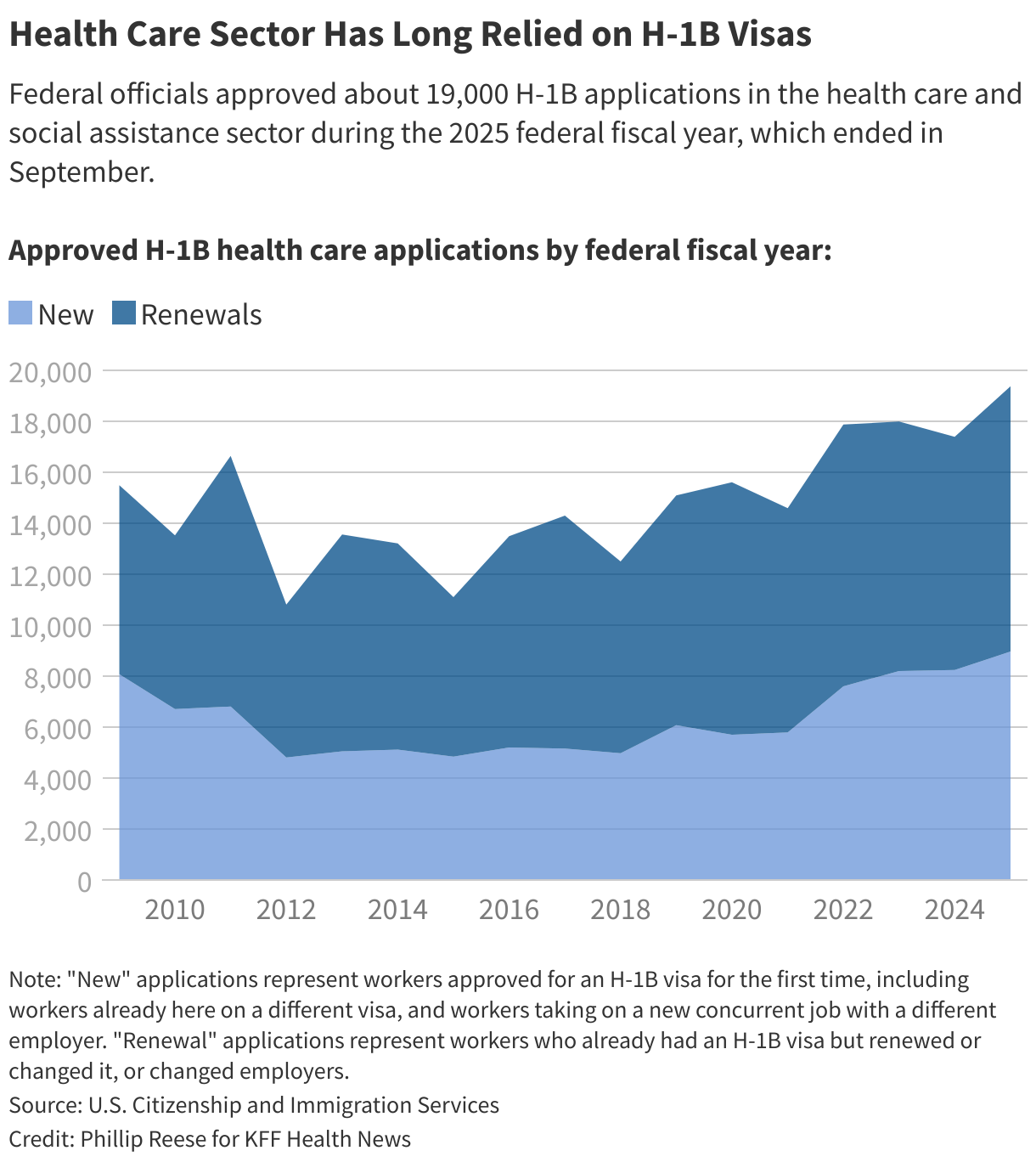
The U.S. health care system depends on foreign-born professionals to fill its ranks of doctors, nurses, technicians, and other health providers, particularly in chronically understaffed facilities in rural America.
But a new presidential proclamation aimed at the tech industry’s use of H-1B visas is making it harder for West River and other rural providers to hire those staffers.
“The health care industry wasn’t even considered. They’re going to be collateral damage, and to such an extreme degree that it was clearly not thought about at all,” said Eram Alam, a Harvard associate professor whose new book examines the history of foreign doctors in the U.S.
Elissa Taub, a Memphis, Tennessee-based attorney who assists hospitals with the H-1B application process, has been hearing concerns from her clients.
“It’s not like there’s a surplus of American physicians or nurses waiting in the wings to fill in those positions,” she said.
Until recently, West River and other employers paid up to $5,000 each time they applied to sponsor an H-1B worker. The visas are reserved for highly skilled foreign workers.
The new $100,000 fee — part of a by President Donald Trump — applies to workers living outside the U.S. but not those who were already in the U.S. on a visa.
West River lab tech Kathrine Abelita is one of nine employees — six technicians and three nurses — at the hospital who are current or former H-1B visa holders. Abelita is from the Philippines and has worked at West River since 2018. She’s now a permanent U.S. resident.
“It’s going to be a big problem for rural health care,” she said of the new fee. She said most younger American workers want to live in urban areas.
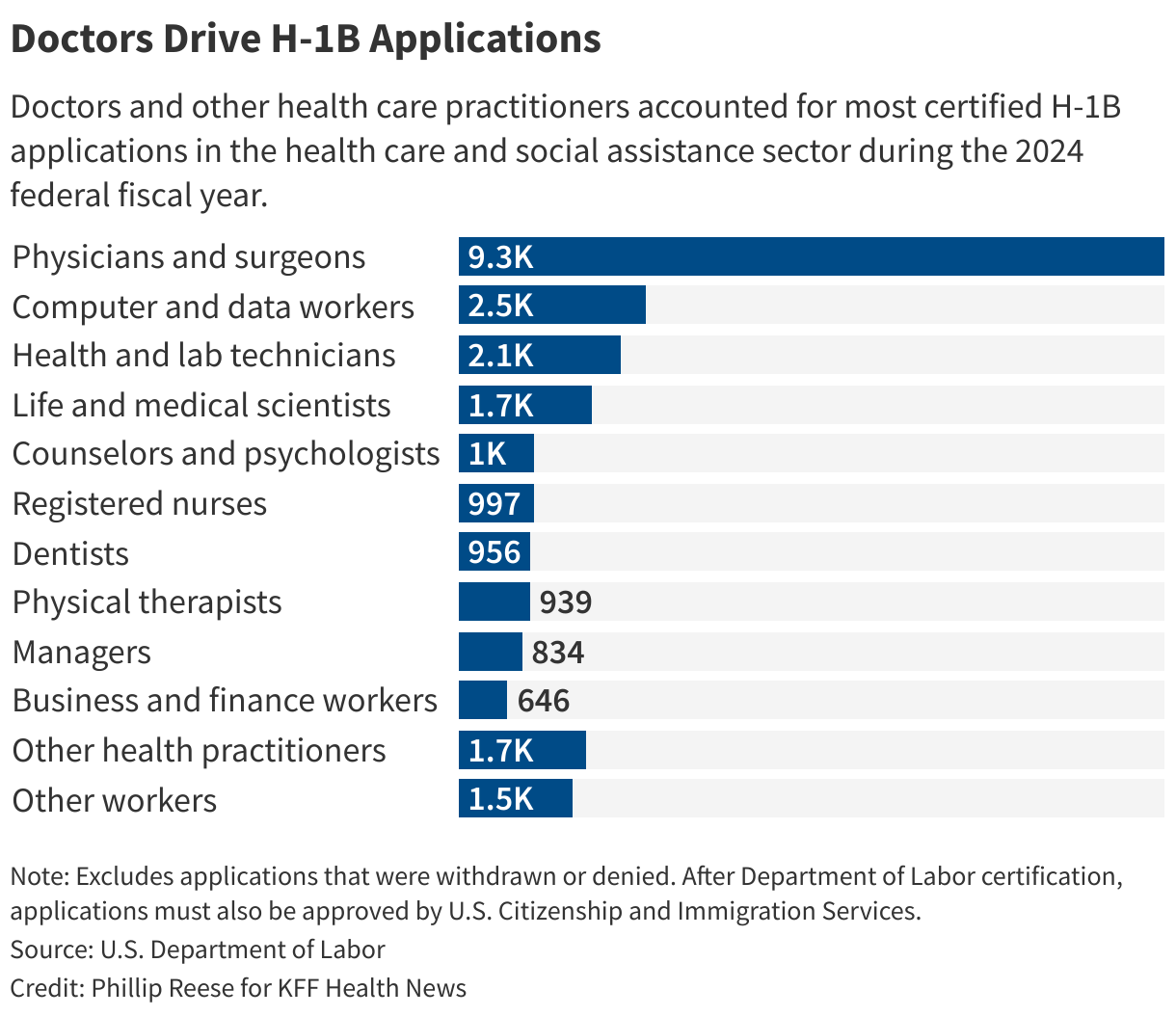
Sixteen percent of registered nurses, 14% of physician assistants, and 14% of nurse practitioners and midwives who work in U.S. hospitals are immigrants, according to a . Nearly a quarter of physicians in the U.S. went to medical school outside the U.S. or Canada, according to .
The , two , and have asked the administration to give the health care industry exemptions from the new fee. The new cost will disproportionally harm rural communities that already struggle to afford and recruit enough providers, the groups argue.
“A blanket exception for healthcare providers is the simplest path forward,” the National Rural Health Association and National Association of Rural Health Clinics wrote in a joint letter.
The proclamation allows fee exemptions for individuals, workers at specific companies, and those in entire industries when “in the national interest.” says the fee will be waived only in an “extraordinarily rare circumstance.” That includes showing that there is “no American worker” available for the position and that requiring a company to spend $100,000 would “significantly undermine” U.S. interests.
Taub called those standards “exceptionally high.”
Representatives of the NRHA and the American Medical Association, which organized a letter from the medical societies, said they’ve received no response after sending requests to Homeland Security Secretary Kristi Noem in late September and early October. The AHA declined to say whether it had heard back.
Homeland Security officials directed Ńîąóĺú´«Ă˝Ň•îl Health News’ inquiries to the White House, which did not answer questions about individual waiver timelines or the possibility of a categorical exemption for the health care industry.
Instead, White House spokesperson Taylor Rogers sent a statement defending the new fee, saying it will “put American workers first.” Her comments echo Trump’s proclamation, which focuses on accusations that the tech industry is abusing the H-1B program by replacing American workers with lower-paid foreign ones. But the order applies to all trades.
Alam, the Harvard professor, said the U.S.’ reliance on international providers does raise legitimate concerns, such as about how it takes professionals away from lower-income countries facing even greater health concerns and staffing shortages than the U.S.
This decades-long dependency, she said, stems from population booms, medical schools’ historical exclusion of nonwhite men, and the “much, much cheaper” cost of importing providers trained abroad than expanding health education in the U.S.
Internationally trained doctors tend to work in rural and urban areas that are poor and underserved, according to and .
Nearly 1,000 H-1B providers were employed in rural areas this year, the two rural health organizations wrote in their letter to the Trump administration.
J-1 visas, the most common type held by foreign doctors during their residencies and other postgraduate training in the U.S., require them to return to their home country for two years before applying for an H-1B.
But a government program called the Conrad 30 Waiver Program allows up to 1,500 J-1 holders a year to remain in the U.S. and apply for an H-1B in exchange for working for three years in a provider shortage area, which includes many rural communities.
Trump’s proclamation says employers that sponsor H-1B workers already inside the U.S., such as doctors with these waivers, won’t have to pay the six-figure fee, a nuance clarified in guidance released about a month later.
But employers will have to pay the new fee when hiring doctors and others who apply while living outside the U.S.
Alyson Kornele, CEO of West River Health Services, said most of the foreign nurses and lab techs it hires are outside the U.S. when they apply.
Ivan Mitchell, CEO of Great Plains Health in North Platte, Nebraska, said most of his hospital’s H-1B physicians were inside the U.S. on other visas when they applied. But he said physical therapists, nurses, and lab techs typically apply from abroad.
Holzkamm said it took five to eight months to hire H-1B applicants at her lab before the new fee was introduced.

Bobby Mukkamala, a surgeon and the president of the American Medical Association, said Republican and Democratic lawmakers are concerned about the ramifications for rural health care.
They include Senate Majority Leader John Thune, who said he planned to reach out about possible exemptions.
“We want to make it easier, not harder, and less expensive, not more expensive, for people who need the workforce,” the Republican told Ńîąóĺú´«Ă˝Ň•îl Health News in September.
Thune’s office did not respond to questions about whether the senator has heard from the administration regarding potential waivers for health workers.
The Trump administration is facing at least two lawsuits attempting to block the new fee. includes a company that recruits foreign nurses and a union that represents medical graduates. , by the U.S. Chamber of Commerce, mentions concerns about the physician shortage and health systems’ ability to afford the new fee.
Kornele said West River won’t be able to afford a $100,000 fee so it’s doubling down on local recruiting and retention.
But Holzkamm said she hasn’t been successful in finding lab techs from North Dakota colleges, even those who intern at the hospital. She said West River can’t compete with the salaries offered in bigger cities.
“It’s a bad cycle right now. We’re in a lot of trouble,” she said.
Phillip Reese is a data reporting specialist and an associate professor of journalism at California State University-Sacramento.
Ńîąóĺú´«Ă˝Ň•îl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/rural-health/h1b-visa-fee-rural-hospitals-foreign-worker-shortages-north-dakota/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=2123805&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>More than three-quarters of American adults didn’t get a covid shot last season, a figure that health care experts warn could rise this year amid new U.S. government recommendations.
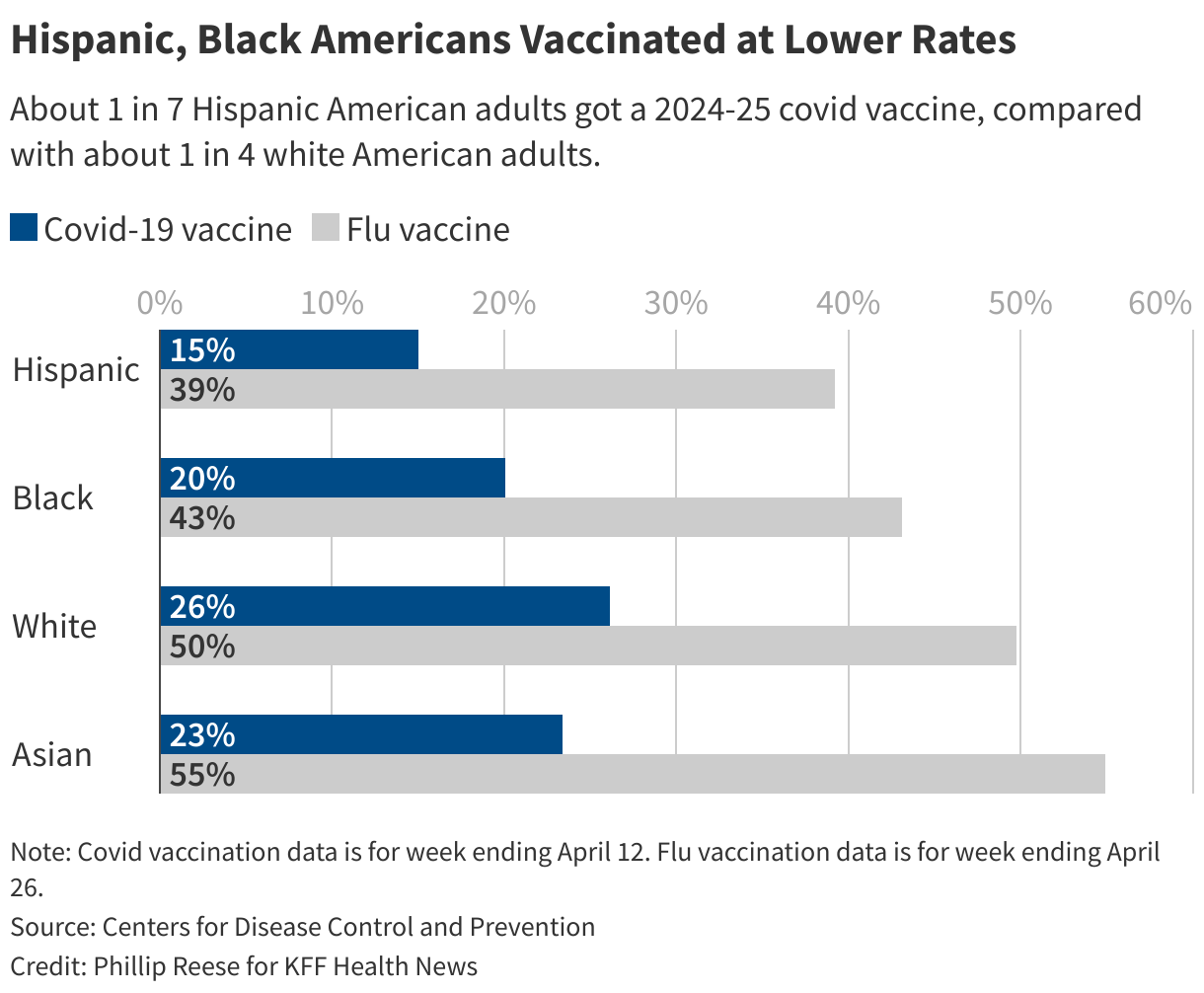
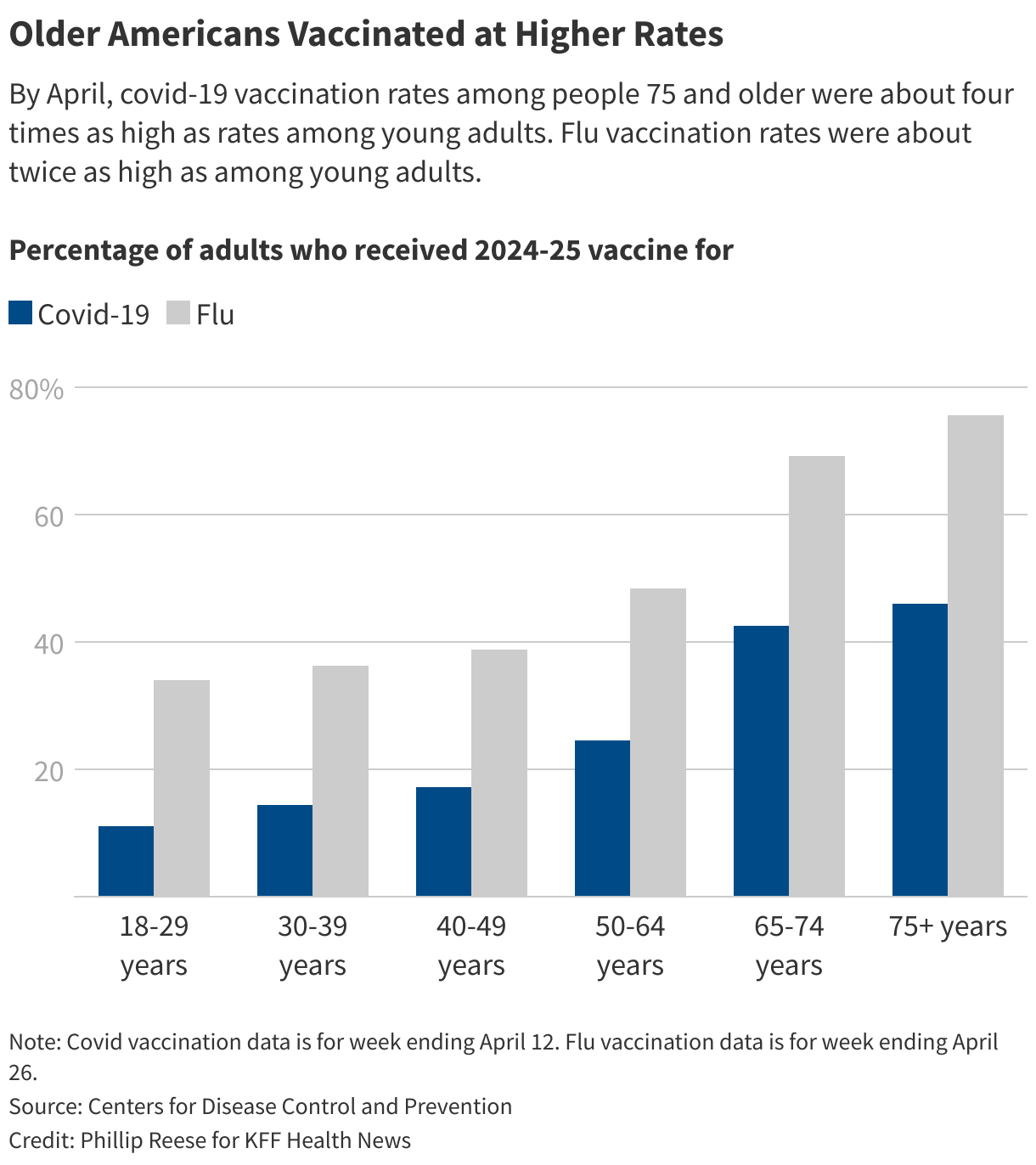
The covid vaccine was initially popular. About 75% of Americans had received of the first versions of the vaccine by early 2022, Centers for Disease Control and Prevention data shows. But only about 23% of American adults got a covid shot during the 2024-25 virus season, well below the 47% of American adults who got a flu shot. The vaccination rates for , , and tetanus are also going down.
Yet covid remains a serious, potentially deadly health risk, listed as the primary cause of death on roughly 31,400 death certificates last year. By comparison, flu killed people and pneumonia, a common complication of the flu, killed , .
As millions of Americans decide whether to get a covid shot this season, public health researchers worry vaccination rates will slide further, especially because Hispanic and Black Americans and those under 30 have lower rates, exposing them to serious complications such as long covid. Under the Trump administration and Health and Human Services Secretary Robert F. Kennedy Jr., the federal government has narrowed its recommendations on the covid vaccine, leading to a hodgepodge of rules on pharmacy access, with Americans living in Republican states often facing more barriers to getting a shot.
“A lot of misinformation is going around regarding covid,” said , an assistant professor of health, society, and behavior at the University of California-Irvine. “Vaccine hesitancy is going to increase.”
In August, the FDA for covid vaccines to those 65 or older and to adults and children with at least one underlying condition that puts them at high risk for serious complications from covid.
A month later, the CDC’s Advisory Committee on Immunization Practices “shared clinical decision-making” on the vaccine, pulling back from advising all adults to get vaccinated. The committee advised doctors to emphasize to adults under 65 and children that the benefits of the vaccine are greatest for those with underlying health conditions.
The guidance is rebutted by infectious disease experts who say most adults and children should get both the flu and covid vaccines, which are safe, effective, and prevent serious illness. Several independent medical organizations like the American Academy of Family Physicians and the American Academy of Pediatrics have reiterated their support for broad adoption of covid vaccines.
More than two dozen states have taken steps to ensure most people can get a covid shot at the pharmacy without a prescription, with many states tying their policies to the advice given by medical organizations. And many of those states require insurers to cover vaccines at no cost, according to . In several other states, predominantly Republican-led, pharmacy access to vaccines may require a prescription.
Among the most commonly cited reasons for covid vaccine hesitation are fears about side effects, long-term health consequences, and the effectiveness of the vaccine, and mistrust of pharmaceutical corporations and government officials, according to of multiple studies, published in the journal Vaccines.
Covid vaccine hesitancy in the 2024-25 virus season was higher among Latinos, African Americans, men, uninsured people, and people living in Republican-leaning states, CDC data shows.
Latino adults were significantly less likely than adults from most other racial and ethnic groups to get a covid shot last season, with a vaccination rate around 15%.
Some of that may be due to age: A of Latinos are young. But public policy actions may also be a factor. The first Trump administration, for example, tied Medicaid to “public charge,” a rule allowing the federal government to deny an immigrant a green card or visa based on their dependence on taxpayer-funded programs. Some Latinos may be afraid to sign up for social services even after the Biden administration reversed those first-term Trump actions.
Haro-Ramos co-authored published in 2024 that found many Latinos were hesitant to get vaccinated because of fears about their immigration status, and that experiencing health discrimination, like care denials or delays, increased their vaccine hesitancy.
“Do you trust the health care system, broadly speaking? Do you want to provide your information — your name, your address?” Haro-Ramos said. “Trust is critical.”
Haro-Ramos said the problem has likely worsened since her study was published. The Trump administration that it would give the personal information of Medicaid enrollees to Immigration and Customs Enforcement. Many Latinos are canceling doctor appointments to head off possible confrontation with immigration enforcement officials.
“People are avoiding leaving their homes at all costs,” Haro-Ramos said.
, an associate professor at the University of Georgia College of Public Health, recently of covid vaccination among nearly 1,500 African Americans living in south Georgia. The study found that participants were more likely to listen to their health care providers than faith leaders or co-workers when seeking advice on getting vaccinated.
More than 90% of those studied had received at least one dose of the vaccine, but those who were unvaccinated were more likely to agree with false statements that tied vaccines to miscarriages, to components’ remaining in the body for a long time, or even to the conspiracy that they implant a computer chip in the body.
“It’s the clinicians who can take the messages about vaccination — that these are myths,” Rajbhandari-Thapa said.
Even though covid hospitalization and death rates have fallen dramatically since the worst days of the pandemic, fatal complications related to covid remain most common among older people. of U.S. covid deaths last year were among people 65 and older, compared with of flu and pneumonia deaths.
As the pandemic falls into the rearview, young people have developed a sense of invincibility. Only 11% of Americans ages 18 to 29 received a vaccine during the 2024-25 virus season, the lowest vaccination rate among adult age groups. That’s far below the who got at least one dose of the initial covid vaccines by November 2023.
While many people get covid after receiving a covid shot, because the vaccine’s ability to prevent infection wears off pretty fast, some misunderstand the purpose of the shot, said , an infectious disease specialist at UCLA Health.
“They think, ‘Well, the vaccine didn’t prevent me from getting covid, so the vaccine didn’t work,’” Yang said. “And what they’re not seeing is that the vaccine prevented them from getting severely ill, which is ultimately the most important thing.”
And the vaccine can help prevent long covid, which is a problem for all ages, Yang said. A recent Northwestern University study younger adults suffer worse symptoms of long covid than older adults.
Ultimately, Yang said, it is not a consistent choice to get a flu vaccine but forgo a covid vaccine, since both are safe, effective, and prevent serious illness. It is clear, he added, that people with compromised immune systems and those at higher risk should get a covid shot. The decision is “a little bit less clear” for others, but “probably most adults should be getting vaccinated, just like it’s recommended for the flu vaccine, as well as most children.”
Phillip Reese is a data reporting specialist and an associate professor of journalism at California State University-Sacramento.
Ńîąóĺú´«Ă˝Ň•îl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-industry/covid-flu-vaccination-rates-virus-season-conflicting-guidance-immigration/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=2110742&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>The health care sector is a bright spot in the economy this year, driving nearly half of the nation’s employment gains, but economists and experts say immigration crackdowns and looming Medicaid cuts pose a threat to future job growth.
Employers from January to August, according to the latest nonfarm payroll data from the Bureau of Labor Statistics. The health care sector of that , expanding by about 232,000 jobs, even though the sector employs only about 11% of workers.
“On the labor side, health care growth is driving the economy,” said Stanford economics professor Neale Mahoney.
Economists say President Donald Trump’s immigration crackdown and cuts to public insurance programs threaten to dampen that growth. They could add unease about the economy and cause headwinds for the GOP in next year’s midterm elections. The health care sector is unusually dependent on foreign-born workers, while a new law trimming federal spending on the $900-billion-a-year Medicaid program is projected, based on a preliminary version of the bill, to trigger the loss of nationwide, according to the Commonwealth Fund.
In recent years, health care job growth has been most pronounced in the home health sector, rising by nearly 300,000 jobs to workers from August 2019 to August 2025, as millions of older residents hire workers to visit and take care of them, Mahoney said. Job growth has also been strong and . Nursing homes and residential care homes from 2019 to 2025 amid an increase in the number of people using caregiving at home.
Some research indicates that health care job growth is not always good for the economy. For instance, a growing number of administrators in health care may raise health care costs to patients. Yet, health care jobs are considered and the health care industry is now the . Even with job growth in the sector, many places for health care workers to meet rising demand.
But several economists said recent federal policy changes on immigration and Medicaid might drag down job growth.
If immigration crackdowns by the Trump administration continue, it could get tough for health care organizations to find enough people to hire. “Health care as an industry is pretty reliant on immigrant labor,” said Allison Shrivastava, an economist with the Indeed Hiring Lab. “It has a large share of non-native labor force, so it’s going to be impacted more.”
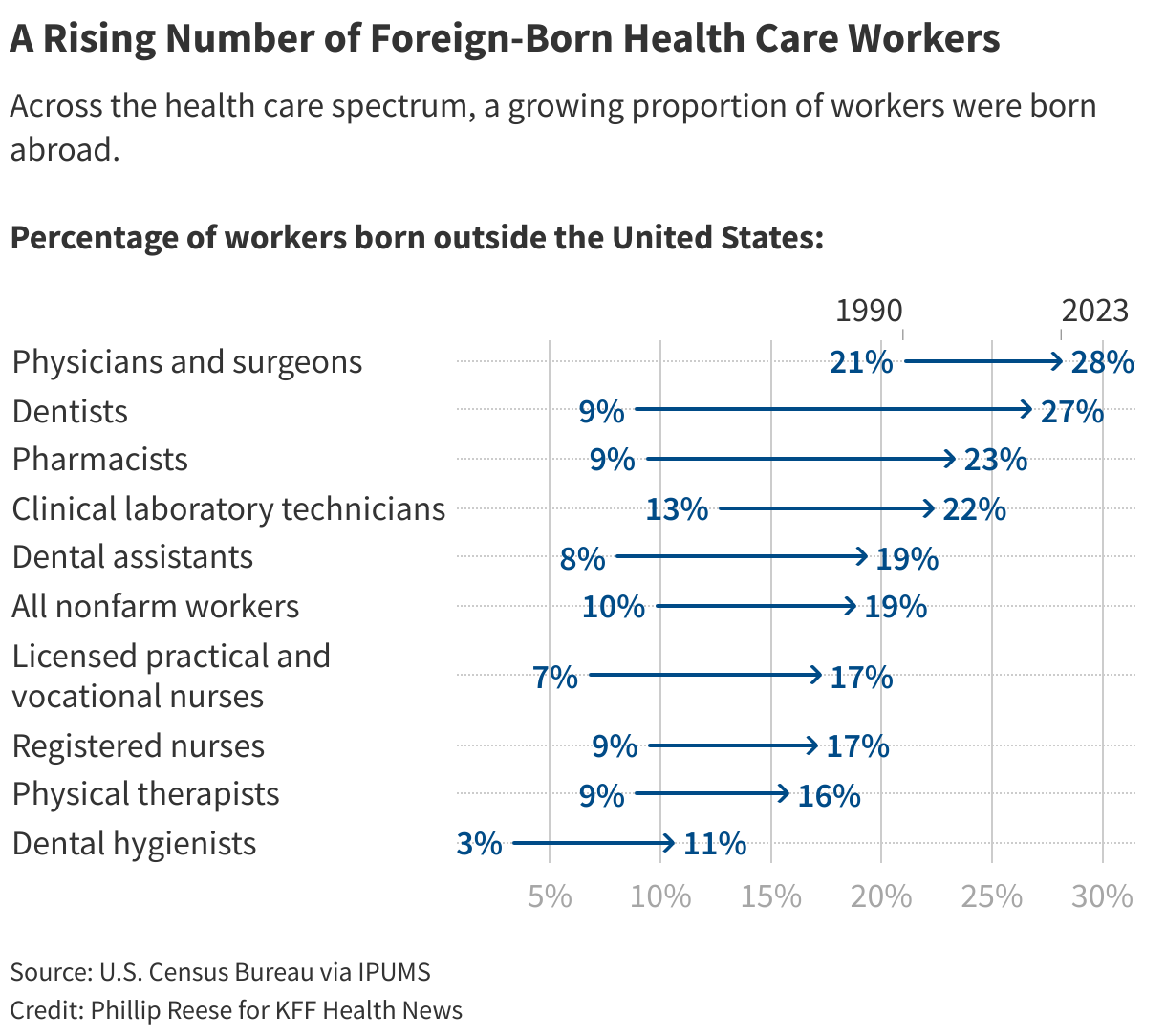
About 18% of Americans employed in health care were born abroad, according to 2023 Census Bureau data. And about 5% of health care workers were not citizens, including about 60,000 doctors and surgeons, 117,000 registered nurses, and 155,000 home health or personal care aides, census data shows.
Many of those workers are here legally; the Census Bureau does not track how many noncitizens are living in the U.S. with authorization. But even those with legal status, including permanent residents, may be vulnerable to deportation. The federal government deported about 200,000 people from February through August, a significant increase from prior months, according to .
At the same time, some health care workers may choose not to study in or move to America if they perceive it as hostile to immigrants. The number of immigrant visas issued by the United States from March to May fell by about 23,000, or 14%, from the same period last year, . In addition, reported unauthorized border crossing attempts .
Shrivastava said Indeed’s job posting data shows continued strong demand for doctors among employers willing to help with the visa sponsorship process. But it’s not clear if people will take them up on the offers.
Meanwhile, Congress this summer passed what Republicans called the “,” which was quickly signed by Trump. That bill makes about $910 billion in cuts to federal Medicaid spending over 10 years, according to of data from the Congressional Budget Office.
Medicaid reductions are projected to cause millions to be without health insurance in the coming years. Hospitals, nursing homes, and community health centers will have to absorb more of the cost of treating uninsured people by reducing services and employees, or else close altogether.
The cuts could have a significant impact on the job market. California alone could see up to 217,000 fewer jobs, of which two-thirds would be in the health care sector, according to by the University of California-Berkeley Labor Center conducted before the bill was finalized and signed.
“It doesn’t mean necessarily that 200,000 people are going to lose their job,” said , interim director of the Health Care Program at the Labor Center. “Some people will lose their job, and in some cases, the job growth won’t be as fast as anticipated.”
Complicating the picture is Trump’s of the official who headed the Labor Department’s statistical branch, leading to concerns that jobs data will not be free from political influence.
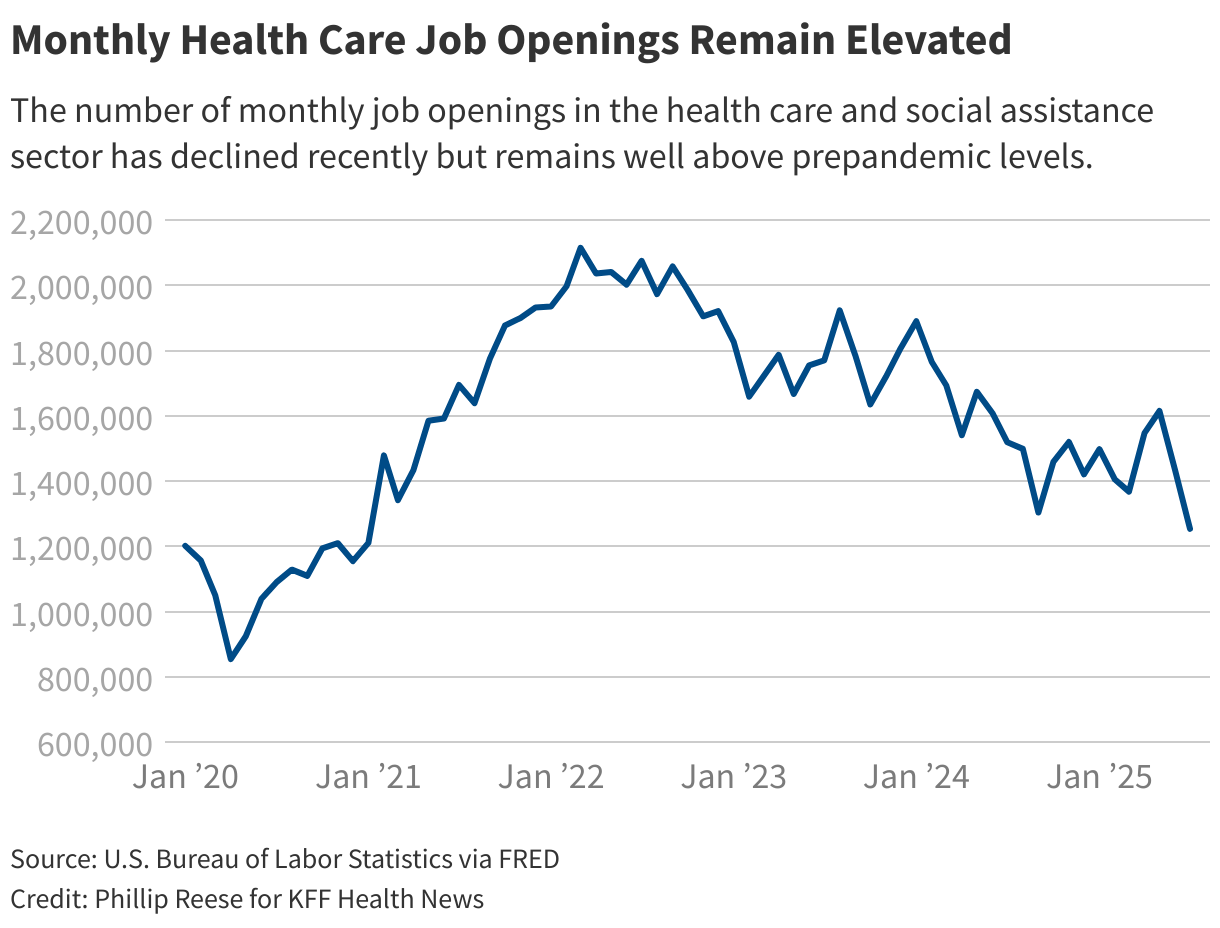
It’s not clear when — or if — immigration actions and Medicaid cuts will affect hiring in the health care sector, but there are signs of potential softening. Federal data showed a in the health care and social assistance sector in July. Indeed’s also shows a decline in some health care fields, but Laura Ullrich, director of economic research in North America at the Indeed Hiring Lab, noted that, overall, postings remain above prepandemic levels.
For now, job growth is expected to remain high, particularly among nurse practitioners, physician assistants, and home health aides, according to .
Many health care jobs require years of higher education but result in high pay, with family physicians typically making and registered nurses typically taking in .
Joshua Lejano, president of the of the California Nursing Students’ Association, said he is “cautiously optimistic” that he will quickly land a job as a registered nurse when he graduates in December. He said he is completing nursing clinical rotations that give him real-world experience that will condition him for long shifts.
Lejano said hospitals in his area are expanding capacity while some veteran nurses are leaving the profession due to burnout from the covid pandemic, creating openings. “Right now, I think the big thing is just staying on top of all the application cycles,” he said.
Health care jobs that don’t require as much training tend to pay much less. Median annual earnings for the U.S.’ roughly 4.4 million home health and personal care aides were last year, roughly equivalent to pay for , federal data shows.
The growth in health care jobs has been especially beneficial for women, Ullrich said. Nearly 80% of health care and social assistance workers are female, according to a recent . The research found that female workers accounted for more than a million new health care jobs in the last two years.
The sector is resilient, Shrivastava said, because Americans generally do not view health care as a luxury good: They pay for it in good times and bad. Health insurance costs are on track for their in at least five years. Also, health care spending often centers on old and very old people, a group growing dramatically as baby boomers age. The number of Americans 65 or older rose from in 1995 to in 2024.
“So many of these health care jobs are to support the growing population of older Americans,” Ullrich said. “So that’s not surprising that we’re seeing growth there. But I think what is surprising is how lopsided it is.”
Phillip Reese is a data reporting specialist and an associate professor of journalism at California State University-Sacramento.
This article was produced by Ńîąóĺú´«Ă˝Ň•îl Health News, which publishes , an editorially independent service of the .
Ńîąóĺú´«Ă˝Ň•îl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-industry/health-care-employment-growth-immigration-crackdown-medicaid-cuts/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
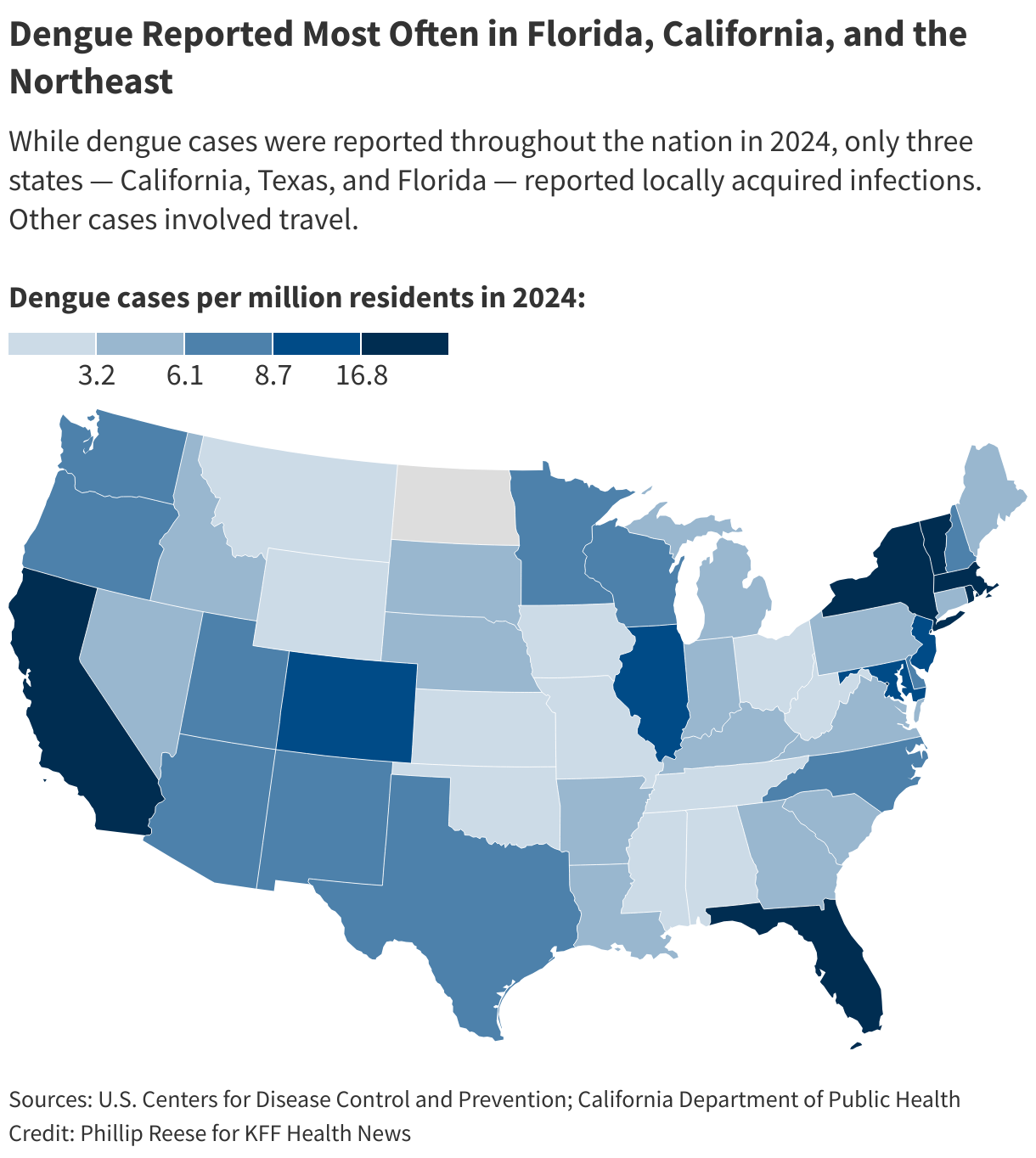
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=2094252&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>As summer ushers in , health and vector control officials are bracing for the possibility of another year of historic rates of dengue. And with climate change, the lack of an effective vaccine, and federal research cuts, they worry the disease will become endemic to a larger swath of North America.
new dengue infections were reported last year in the contiguous United States, up from about 2,050 in 2023, according to the Centers for Disease Control and Prevention. All of last year’s cases were acquired abroad, except for 105 cases contracted in California, Florida, or Texas. The CDC issued a in March warning of the ongoing risk of dengue infection.
“I think dengue is here with us to stay,” said infectious disease specialist associate medical director of hospital epidemiology at in Los Angeles, about dengue becoming a new normal in the U.S. “These mosquitoes aren’t going anywhere.”
Dengue is endemic — a label health officials assign when diseases appear consistently in a region — in of the world, including Latin America, India, and Southeast Asia. Dengue cases in many of those places, especially in Central and South America.
The disease, which when people are bitten by infected Aedes mosquitoes, was not common in the contiguous United States for much of the last century. Today, most locally acquired (meaning unrelated to travel) dengue cases in the U.S. happen in Puerto Rico, which saw a sharp increase , triggering a local public health emergency.
Most people who contract dengue . But in some people symptoms are severe: bleeding from the nose or mouth, intense stomach pain, vomiting, and swelling. Occasionally, dengue causes death.
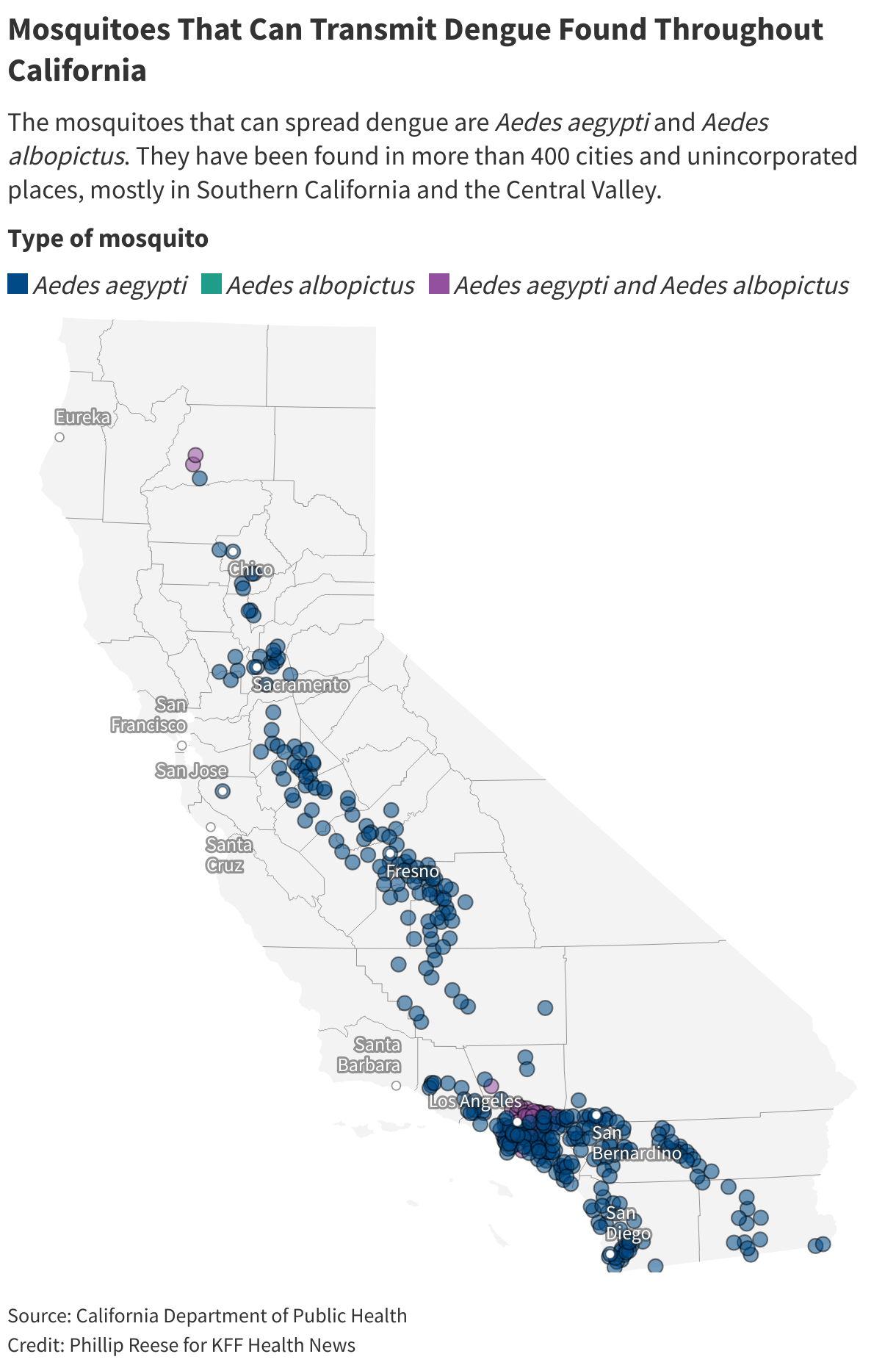
California offers a case study in how dengue is spreading in the U.S. The Aedes aegypti and Aedes albopictus mosquitoes that transmit dengue weren’t known to be in the state . They are now found in 25 counties and and unincorporated communities, mostly in Southern California and the Central Valley.
The spread of the mosquitoes is concerning because their presence increases the likelihood of disease transmission, said Steve Abshier, president of the .
From 2016 through 2022, there were an average of 136 new dengue cases a year in California, each case most likely brought to the state by someone who had traveled and been infected elsewhere. In 2023, there were about 250 new cases, including two acquired locally.
In 2024, California saw 725 new dengue cases, including 18 acquired locally, .
Climate change could contribute to growth in the Aedes mosquitoes’ population, Ben-Aderet said. These mosquitoes survive best in warm urban areas, often biting during the daytime. Locally acquired infections often occur when someone catches dengue during travel, then comes home and is bitten by an Aedes mosquito that bites and infects another person.
“They’ve just been spreading like wildfire throughout California,” Ben-Aderet said.
Dengue presents a challenge to the many primary care doctors who have never seen it. Ben-Aderet said doctors who suspect dengue should obtain a detailed travel history from their patients, but confirming the diagnosis is not always quick.
“There’s no easy test for it,” he said. “The only test that we have for dengue is antibody tests.” He added that “most labs probably aren’t doing it commercially, so it’s usually like a send-out test from most labs. So you really have to suspect someone has dengue.”
Best practices for avoiding dengue include eliminating any standing pools of water on a property — even small pools — and using mosquito repellent, Abshier said. Limiting activity at dusk and dawn, when mosquitoes bite most often, can also help.
Efforts to combat dengue in California became even more complicated this year after wildfires ripped through Los Angeles. The fires occurred in a hot spot for mosquito-borne illnesses. San Gabriel Valley Mosquito and Vector Control District officials for months to treat more than 1,400 unmaintained swimming pools left in the wake of fire, removing potential breeding grounds for mosquitoes.
San Gabriel vector control officials have used local and state resources to treat the pools, said district spokesperson Anais Medina Diaz. They have applied for reimbursement from the Federal Emergency Management Agency, which has not historically paid for vector control efforts following wildfires.
In California, vector control agencies are often primarily funded by local taxes and fees on property owners.
Some officials are pursuing the novel method of to reduce the problem. That may prove effective, but deploying the method in a large number of areas would be costly and would require a massive effort at the state level, Abshier said. Meanwhile, the federal government is pulling back on interventions: Several outlets have reported that the National Institutes of Health will new climate change-related research, which could include work on dengue.
This year, reported rates of dengue in much of the Americas from 2024. But the trend in the United States likely won’t be clear until later in the year, after the summer mosquito season ends.
Health and vector control researchers aren’t sure how bad it will get in California. Some say there may be limited outbreaks, while others predict dengue could get much worse. , a professor and infectious disease researcher at the La Jolla Institute for Immunology, said other places, like Nepal, experienced relatively few cases of dengue in the recent past but now regularly see large outbreaks.
There is a vaccine for children, but it from a lack of global demand. Two other dengue vaccines are unavailable in the United States. Shresta’s lab is hard at work on for dengue. She hopes to release results from animal testing in a year or so; if the results are positive, human trials could be possible in about two years.
“If there’s no good vaccine, no good antivirals, this will be a dengue-endemic country,” she said.
Phillip Reese is a data reporting specialist and an associate professor of journalism at California State University-Sacramento.
This article was produced by Ńîąóĺú´«Ă˝Ň•îl Health News, which publishes , an editorially independent service of the .
Ńîąóĺú´«Ă˝Ň•îl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/public-health/mosquito-season-new-normal-dengue-vaccine-florida-california-climate-change/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=2054080&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>While patients and providers say teletherapy is effective and easier to get than in-person services, experts in the field noted that teletherapy often requires a skilled mental health practitioner trained to pick up subtle communication cues.
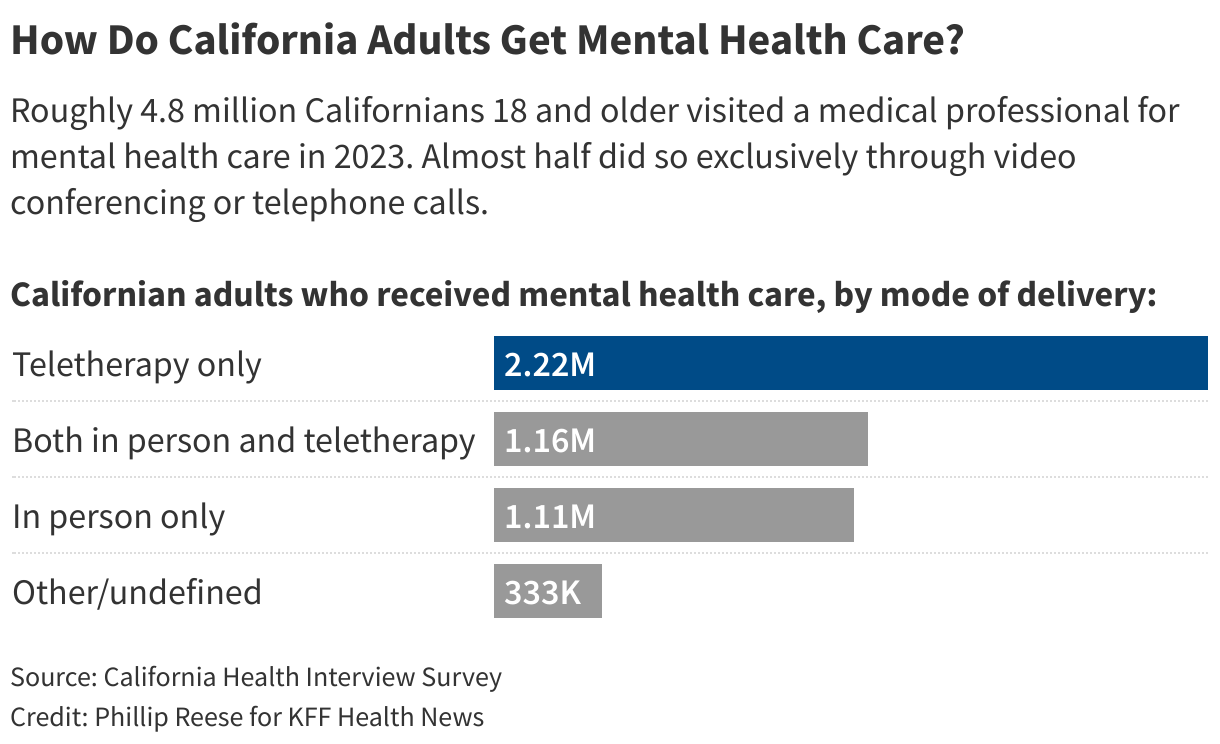
Almost half of the roughly 4.8 million adults who visited a medical professional for mental health or substance use disorders in 2023 did so exclusively through teletherapy, according to a Ńîąóĺú´«Ă˝Ň•îl Health News analysis of the latest data from UCLA’s .
About 24% of adults used a combination of face-to-face and teletherapy in 2023, while roughly 23% got help exclusively in person, according to the survey of about 20,000 California households.
A of patients in the Department of Veterans Affairs health care system found a similar pattern: Fifty-five percent of mental health care continued to be provided via telemedicine, a figure that spiked after patients shifted to teletherapy by necessity during the covid-19 pandemic.
Teletherapy is certainly more convenient, allowing patients to see their therapists from the comfort of home.
“It’s actually really effective,” said , president of the . “I think part of that is that it just allows more comfortability — people are willing to work a little bit more when they’re comfortable.”
: Teletherapy patients report getting better at rates similar to those receiving in-person therapy.
“Research has basically shown that there’s no difference between teletherapy versus in-person therapy — so, basically, as effective as in-person therapy,” said , a researcher at the , who recently conducted an analysis of several studies comparing teletherapy and face-to-face therapy.
But Lin said it can be difficult for a therapist to see hand motions or read body language during a video call, which could lead to therapists missing nonverbal cues about their patients’ emotional states. Lin’s most recent research, yet to be published, suggests therapy over the telephone “is less effective than video conferences” due to “more loss of information.”
And some people have trouble emotionally connecting with a therapist without seeing them in person, Lin said. Technical difficulties, not uncommon, can also interfere with clients building a therapeutic relationship.
Sacramento resident David Bain relies on teletherapy to treat his depression because mobility issues make it difficult for him to visit a therapist in person.
“It’s almost to the point where I wouldn’t be able to get the service if I wasn’t able to get it through telehealth,” said Bain, executive director of , a nonprofit that provides support and advocacy to people with mental illness.
Bain said that his one-on-one teletherapy sessions have helped but that he’s had less success with online group therapy. He recently participated in a 10-week therapy class, but he didn’t get the connection and support he received in past in-person group settings, he said.
“There was probably me and two or three other people that were actually showing ourselves on screen,” he said. “Everyone else had their screens off.”
Teletherapy is increasingly offered through cellphone applications like and . Patients using these applications often pay a subscription fee, which insurance may partly cover, in exchange for regular sessions and contact with therapists.
, a researcher at the , co-authored published in 2023 that looked at patient reviews of eight of the most popular teletherapy apps. Many patients expressed satisfaction with their therapists, but the team also uncovered negative patterns.
Some patients did not get the therapy they paid for, often due to technical difficulties. Other patients reported their therapists acted disinterested or unprofessional, a finding Jo said could be tied to the relatively low pay therapists earn on some apps.
And several users mentioned in reviews that their therapist suddenly disappeared from the app without explanation. She said therapists in more traditional “pay-as-you-go” arrangements rarely discontinue treatment without warning.
, chief medical officer of Talkspace, said patients often can use their insurance to get therapy on the platform, at a typical cost of a $10 copay. Separately, Talkspace spokesperson Jeannine Feyen said salary for therapists has increased since Jo’s study was conducted, and that full-time Talkspace therapists make between $65,000 and $105,000 a year.
At BetterHelp, therapists earn up to $91,000 and the average patient rating last year for a live session on the platform was , spokesperson Megan Garner said. A significant majority of patients reported reliable symptom improvement or remission, she added.
The number of Californians visiting a medical professional for mental health issues rose by about 434,000, or 10%, from 2019 to 2023, UCLA data shows. It jumped by nearly 2 million, or 69%, from 2009 through 2023.
Even so, the transition from in-person therapy to teletherapy has left some behind.
The UCLA data shows that Californians living within 200% of the federal poverty level — for example, a family of four with a household income of about $60,000 or under in 2023 — were less likely to use teletherapy.
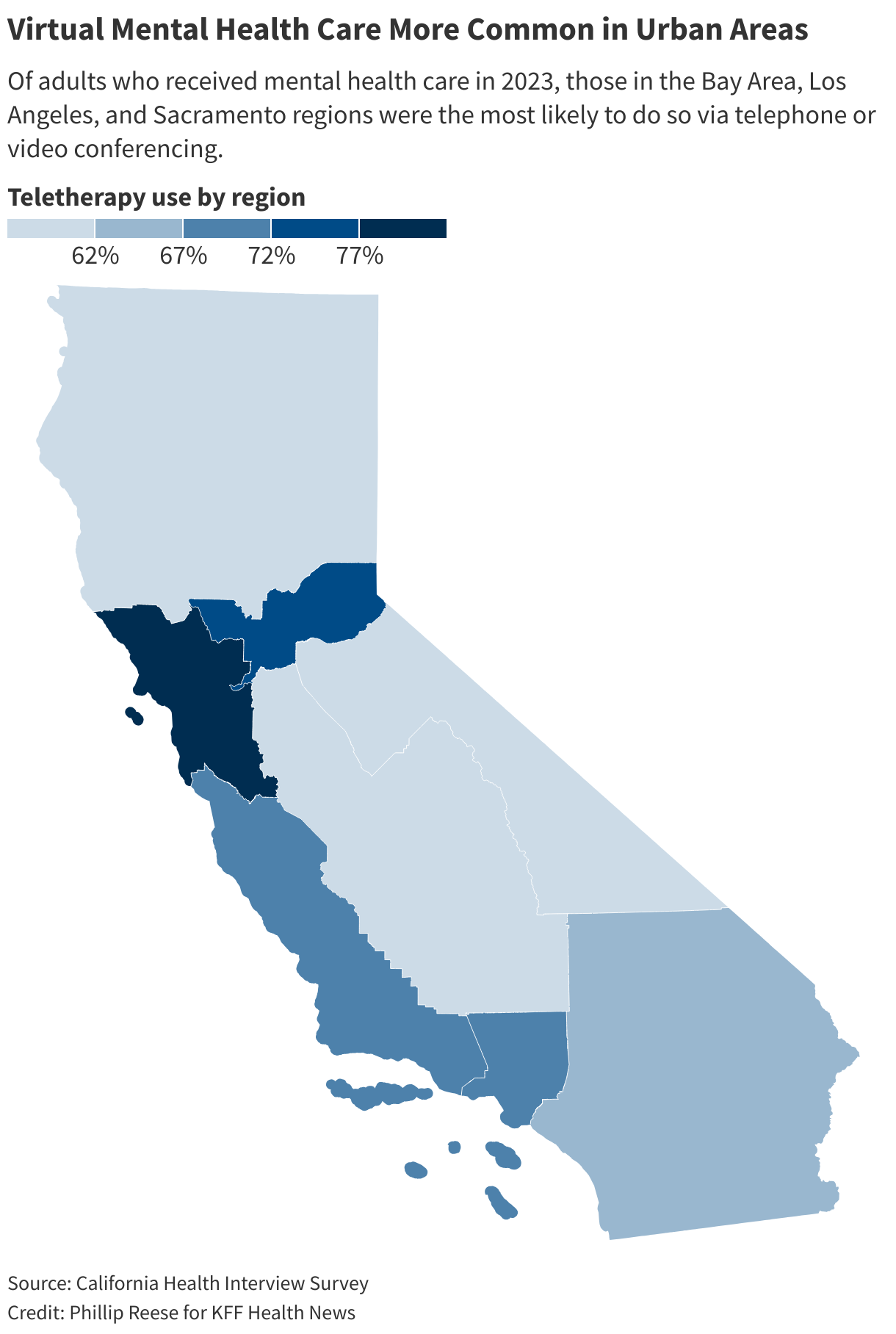
The data also shows that residents in rural areas, where access to telehealth should provide a boon, weren’t using it as much as residents of urban areas.
For example, about 81% of Bay Area residents who visited a medical professional for mental health care in 2023 did so either fully or partially via teletherapy. About 62% of residents in the state’s rural, mountainous counties did the same.
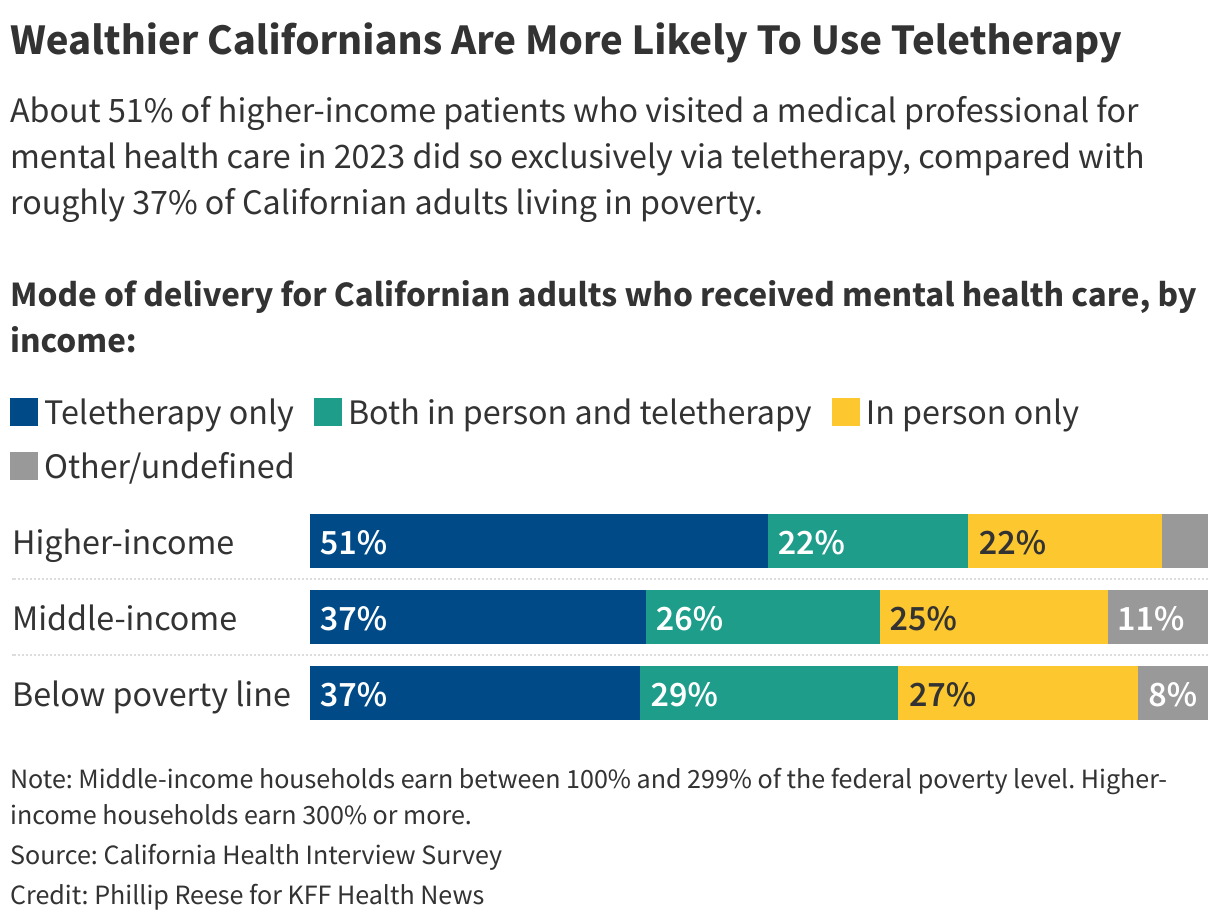
Those disparities are suggestive of gaps seen in remote-work patterns: Wealthier, urban Californians are more likely to work from home than residents. By extension, Californians of greater means have more opportunities to arrange online appointments and may be more comfortable with them.
By comparison, low-income folks tend to go into the office for doctor visits, Heitzmann said.
Lower-income and rural Californians may also lack the reliable internet service necessary for good telehealth. A recent Ńîąóĺú´«Ă˝Ň•îl Health News analysis found millions of Americans live in places with doctor shortages and poor internet access.
Lower-income Californians also , making privacy for an intimate therapy session difficult.
Regardless, teletherapy is now dominant. And it’s not just patients who enjoy the convenience. Many therapists have ditched expensive office rents to work from home.
“Covid allowed that,” Heitzmann said. “A lot of folks really just got rid of their offices and were perfectly happy converting their home into some kind of office and doing it all day long.”
This article was produced by Ńîąóĺú´«Ă˝Ň•îl Health News, which publishes , an editorially independent service of the .
Ńîąóĺú´«Ă˝Ň•îl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-industry/mental-health-substance-misuse-treatment-video-chat-phone-call-teletherapy-california/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=2030883&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>“It’s for the two of us, and we’re not sick,” said Vartan, general manager at pizza shops in the Bay Area cities of San Jose and Sunnyvale. “It’s ridiculous.”
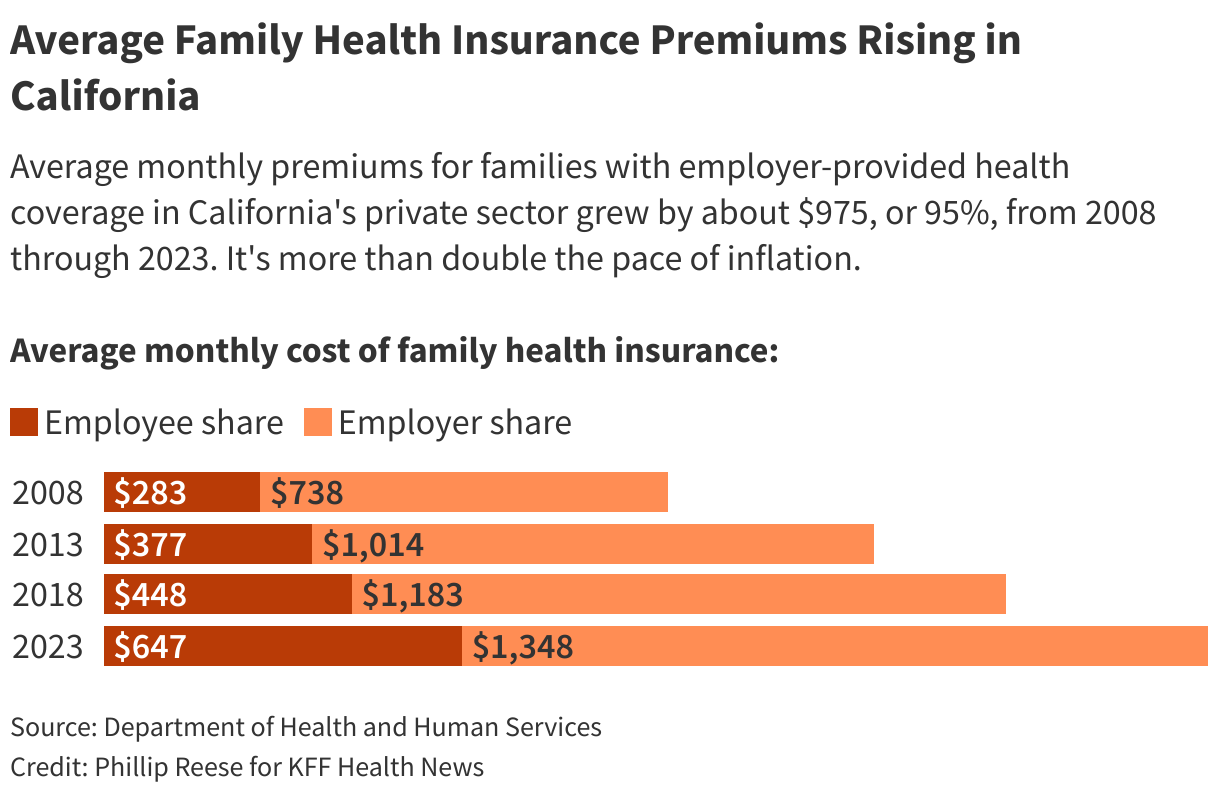
Vartan, who is in his late 50s, is one of millions of Californians struggling to keep up with health insurance premiums ballooning faster than inflation.
Average monthly premiums for families with employer-provided health coverage in California’s private sector nearly doubled over the last 15 years, from just over $1,000 in 2008 to almost $2,000 in 2023, a Ńîąóĺú´«Ă˝Ň•îl Health News analysis of . That’s more than twice the rate of inflation. Also, employees have had to absorb a growing share of the cost.
The spike is not confined to California. Average premiums for families with employer-provided health coverage grew as fast nationwide as they did in California from 2008 through 2023, . Premiums in 2024, according to KFF.
Small-business groups warn that, for workers whose employers don’t provide coverage, the problem could get worse if Congress does not extend that make health insurance more affordable on individual markets such as Covered California, the public marketplace that insures more than 1.9 million Californians.
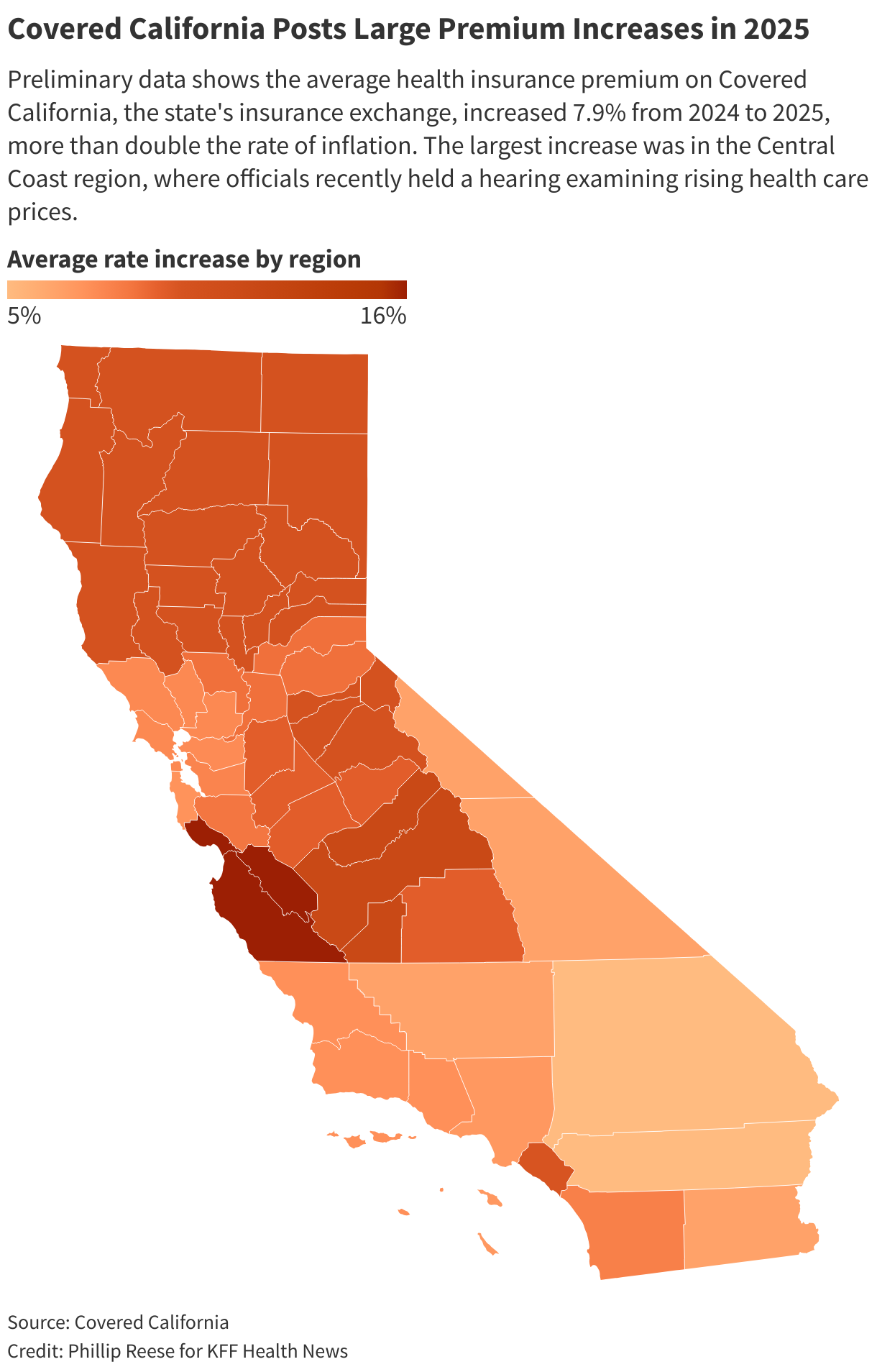
Premiums on Covered California have since 2022, roughly double the pace of inflation. But the exchange helps nearly 90% of enrollees mitigate high costs by offering state and federal , with many families paying little or nothing.
Rising premiums also have hit government workers — and taxpayers. Premiums at CalPERS, which provides insurance to more than 1.5 million of California’s active and retired public employees and family members, . Public employers pay part of the cost of premiums as negotiated with labor unions; workers pay the rest.
“Insurance premiums have been going up faster than wages over the last 20 years,” said , a researcher at the who focuses on health insurance. “Especially in the last couple of years, those premium increases have been pretty dramatic.”
Dietz said rising hospital prices are largely to blame. Consumer costs for hospitals and nursing homes rose about 88% from 2009 through 2024, roughly double the overall inflation rate, according to data from the . The rising cost of administering America’s massive health care system has also pushed premiums higher, she said.
Insurance companies remain highly profitable, but their gross margins — the amount by which premium income exceeds claims costs — were fairly steady during the last few years, . Under federal rules, insurers percentage of premiums on medical care.
Rising insurance costs are cutting deeper into family incomes and squeezing small businesses.
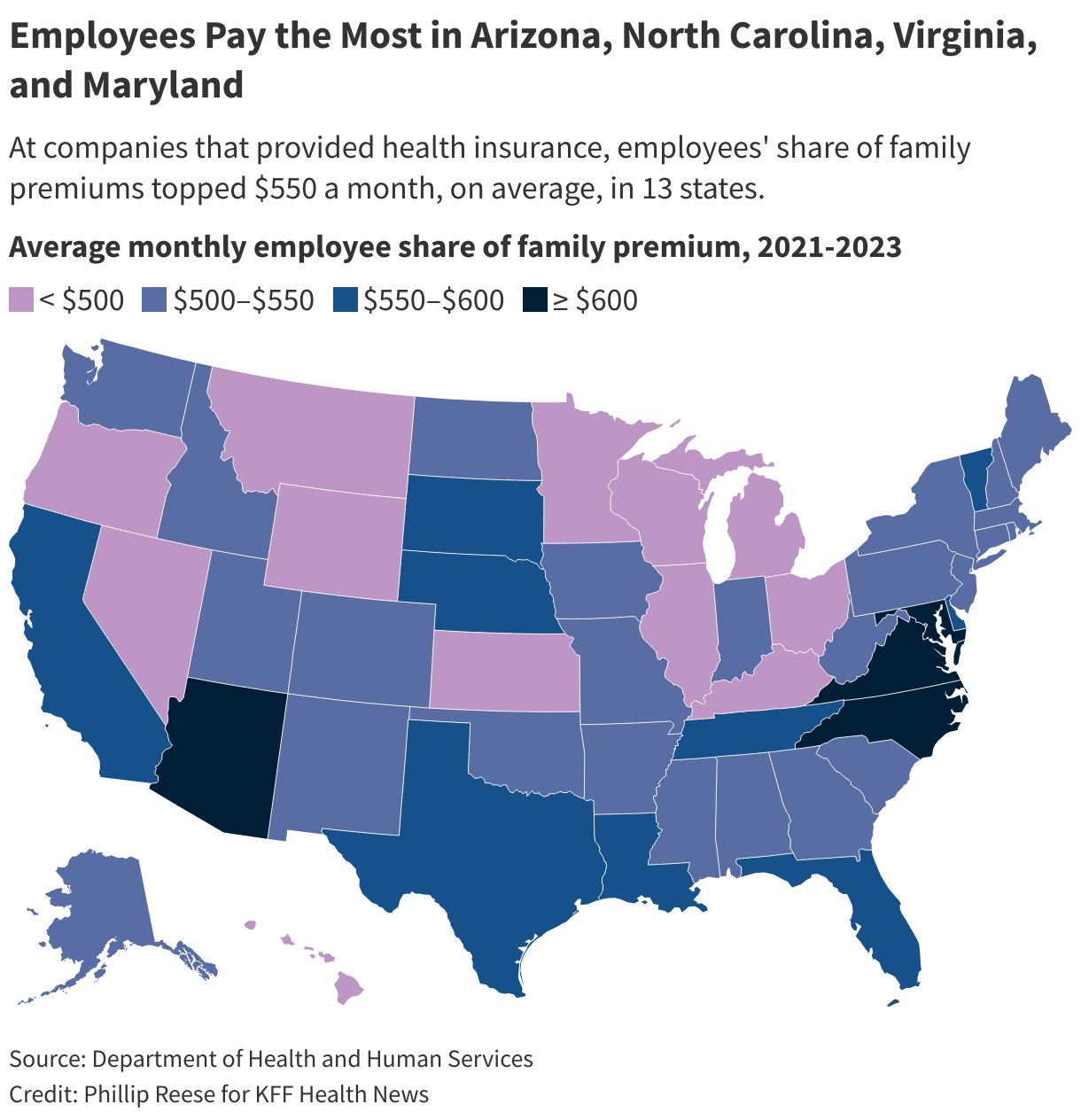
The average annual cost of family health insurance offered by private sector companies was about $24,000, or roughly $2,000 a month, in California during 2023, according to the . Employers paid, on average, about two-thirds of the bill, with workers paying the remaining third, about $650 a month. Workers’ share of premiums has grown faster in California than in the rest of the nation.
Many small-business workers whose employers don’t offer health care turn to Covered California. During the last three decades, the percentage of businesses nationwide with 10 to 24 workers offering health insurance fell from 65% to 52%, according to the . Coverage fell from 34% to 23% among businesses with fewer than 10 employees.
“When an employee of a small business isn’t able to access health insurance with their employer, they’re more likely to leave that employer,” said , California director for , an advocacy group representing more than 85,000 small businesses across America.
Kirk Vartan said his pizza shop employs about 25 people and operates as a worker cooperative — a business owned by its workers. The small business lacks negotiating power to demand discounts from insurance companies to cover its workers. The best the shop could do, he said, were expensive plans that would make it hard for the cooperative to operate. And those plans would not offer as much coverage as workers could find for themselves through Covered California.
“It was a lose-lose all the way around,” he said.
Mark Seelig, a spokesperson for Blue Shield of California, said rising costs for hospital stays, doctor visits, and prescription drugs put upward pressure on premiums. Blue Shield has created that he said is designed to lower drug prices and pass on savings to consumers.
Even at California companies offering insurance, the percentage of employees enrolled in plans with a deductible has roughly doubled in 20 years, rising to 77%, federal data shows. Deductibles are the amount a worker must pay for most types of care before their insurance company starts paying part of the bill. The average annual deductible for an employer-provided family health insurance plan was about $3,200 in 2023.
During the last two decades, the cost of health insurance premiums and deductibles in California rose from about 4% of median household income , according to the UC Berkeley Labor Center, which conducts research on labor and employment issues.
As a result, the center found, many Californians are choosing to delay or forgo health care, including some preventive care.
California is trying to lower health care costs by setting statewide spending growth caps, which state officials hope will curb premium increases. The state recently established the , which set a five-year target for annual spending growth , dropping to 3% by 2029. Failure to hit targets could result in hefty fines for health care organizations, though that likely wouldn’t happen until 2030 or later.
Other states that imposed similar caps saw health care costs rise more slowly than states that did not, Dietz said.
“Does that mean that health care becomes affordable for people?” she asked. “No. It means it doesn’t get worse as quickly.”
This article was produced by Ńîąóĺú´«Ă˝Ň•îl Health News, which publishes , an editorially independent service of the .
Ńîąóĺú´«Ă˝Ň•îl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-care-costs/california-health-insurance-premium-costs-exceed-inflation-data-dataviz/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1995430&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>SACRAMENTO, Calif. — A growing number of people — many of them older and homeless — are freezing to death during winter.
Hypothermia from exposure to cold temperatures was the underlying or contributing cause of death for 166 Californians last year, more than double the number a decade ago, according to from the U.S. Centers for Disease Control and Prevention. The age-adjusted rate of 3.7 deaths per million residents in 2023 was the highest in the state in at least 25 years.
Hypothermia deaths have also increased nationwide, with about 2,520 Americans dying last year, up about 35% from 2014, . It was even worse in 2022: 3,500 hypothermia deaths, many of them during brutal winter storms across much of the country in and .
The increase in hypothermia deaths is linked to a , especially in California, which has the nation’s largest homeless population, experts say.
Homeless people are particularly susceptible to hypothermia because so many older, vulnerable adults live outside, where they are exposed to the elements. Government officials have largely responded to hypothermia deaths by opening warming centers where homeless people can stay on cold nights, but advocates say more permanent housing and more programs that prevent homelessness are needed.
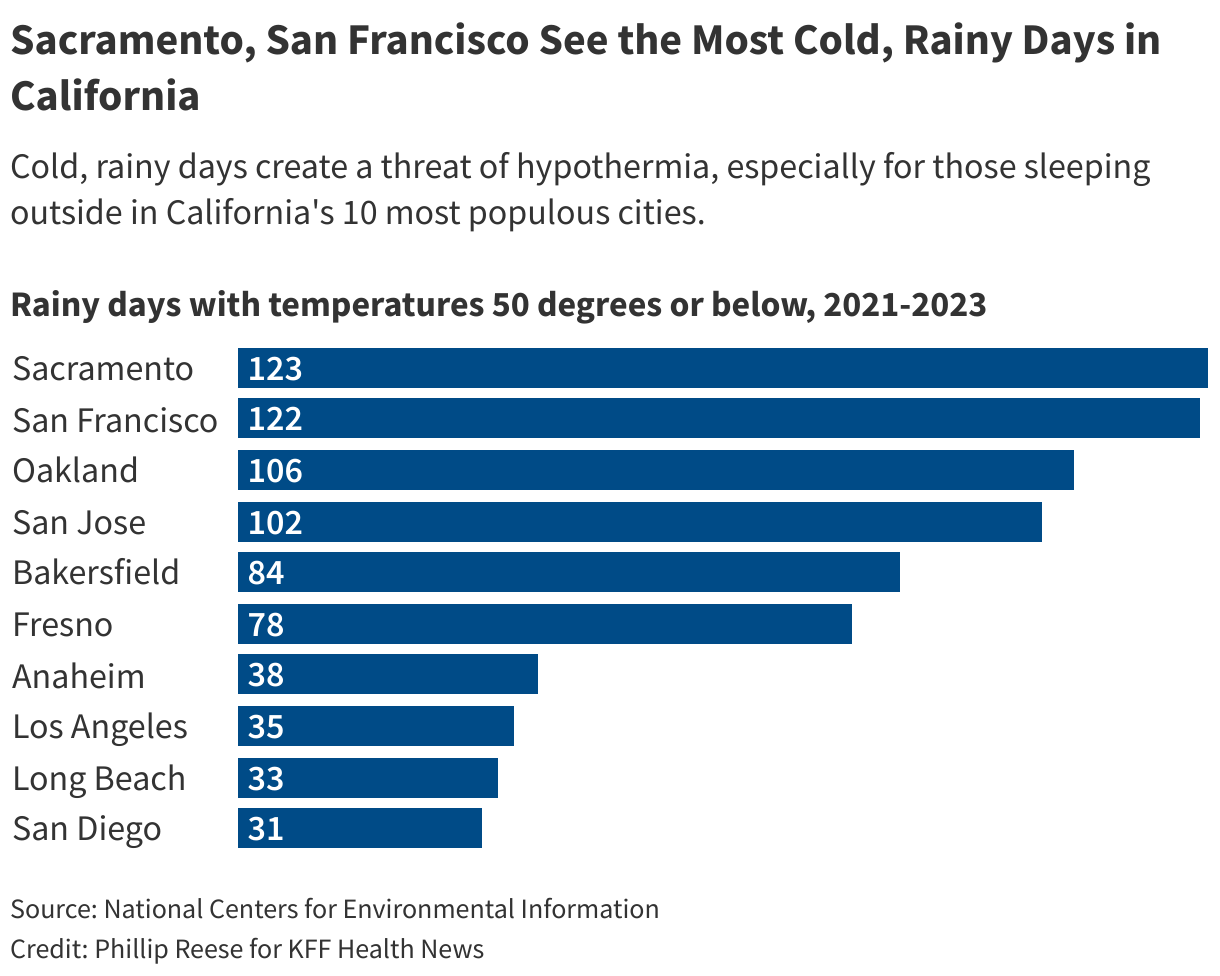
Sitting on a park bench near the state Capitol, Leon Winch said he has trouble staying warm as winter approaches. On cold, rainy nights, he tries to find places to stay dry but covered spots are often patrolled by private security guards who chase him away. Hypothermia often occurs in cold temperatures below 40 degrees but at warmer temperatures, especially when it’s rainy.
City officials open centers , including when nightime temperatures are likely to fall below 37 degrees on two or more days in a five-day period. But Winch said he does not trust the city of Sacramento and doesn’t use the city’s warming centers even as temperatures grow frigid.
“They’re not doing anything except window-dressing,” he said.
According to the California Department of Health Care Access and Information, homeless people accounted for 18% of hospitalizations and emergency room visits related to hypothermia from 2019 through 2023. Homeless Californians represent nearly 0.5% of the state’s population, suggesting they are about 40 times as likely as others to end up at the hospital for hypothermia.
Federal data shows more than two-thirds of the state’s 181,000 homeless people are unsheltered. And among those dying from hypothermia, one group has been hit particularly hard.
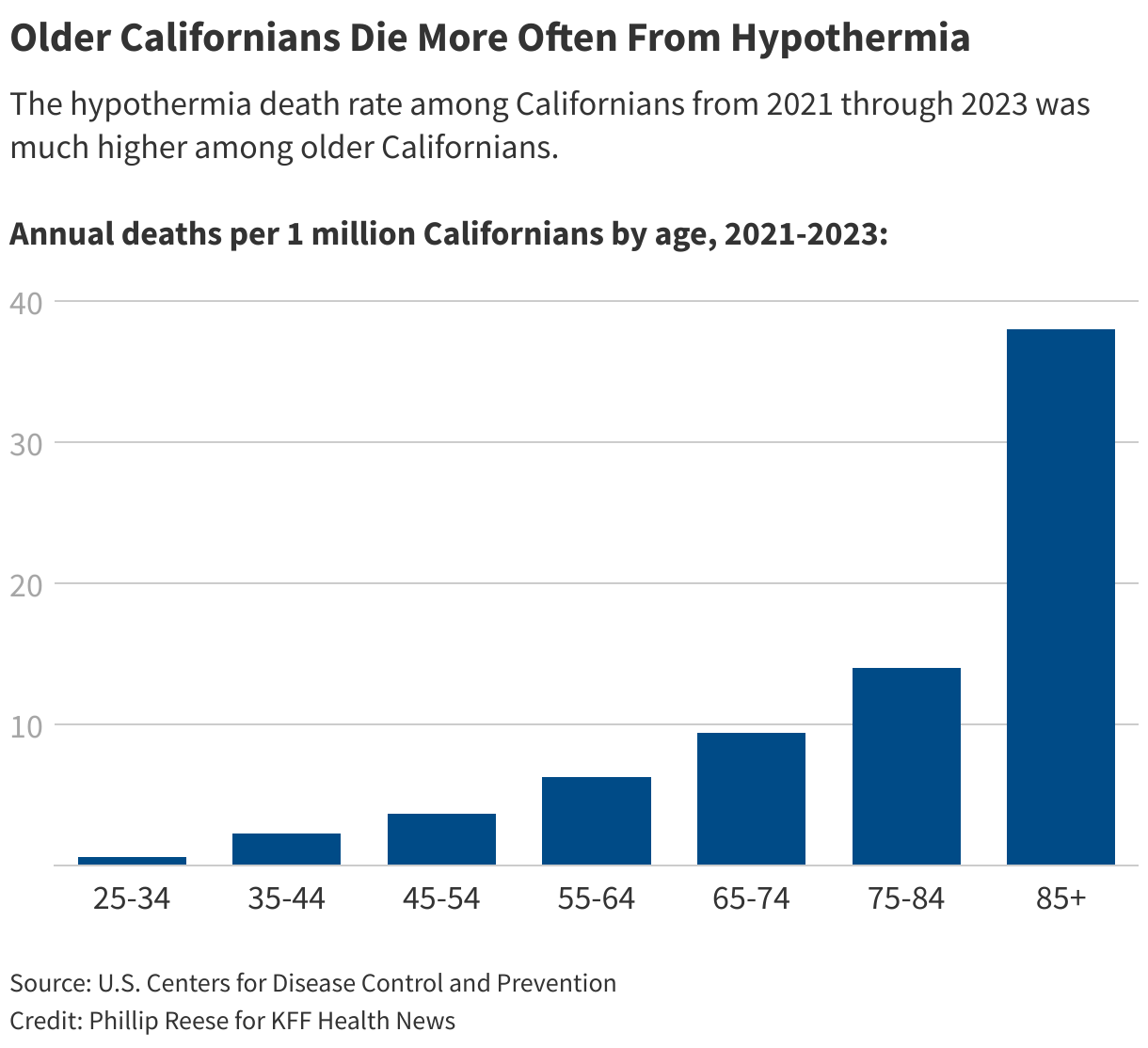
Older adults are most susceptible to hypothermia, with people 55 and older accounting for more than three-quarters of hypothermia deaths in California from 2021 through 2023, .
“There is a massive increase in the aging homeless population,” said , director of the University of California-San Francisco . She said the proportion of single homeless adult Californians who are 50 or older has increased from 11% in 1990 to .
And as the number of deaths from exposure to cold has risen in the state, so has the number of deaths from exposure to heat in the summer. “A changing climate, more temperature extremes, more soaking rains — people are older and thus unable to even tolerate it, so they get much sicker, faster,” Kushel said.
The trend could worsen: The proportion of the homeless population 65 or older is projected to triple in the United States between 2017 and 2030, according to UCSF researchers.
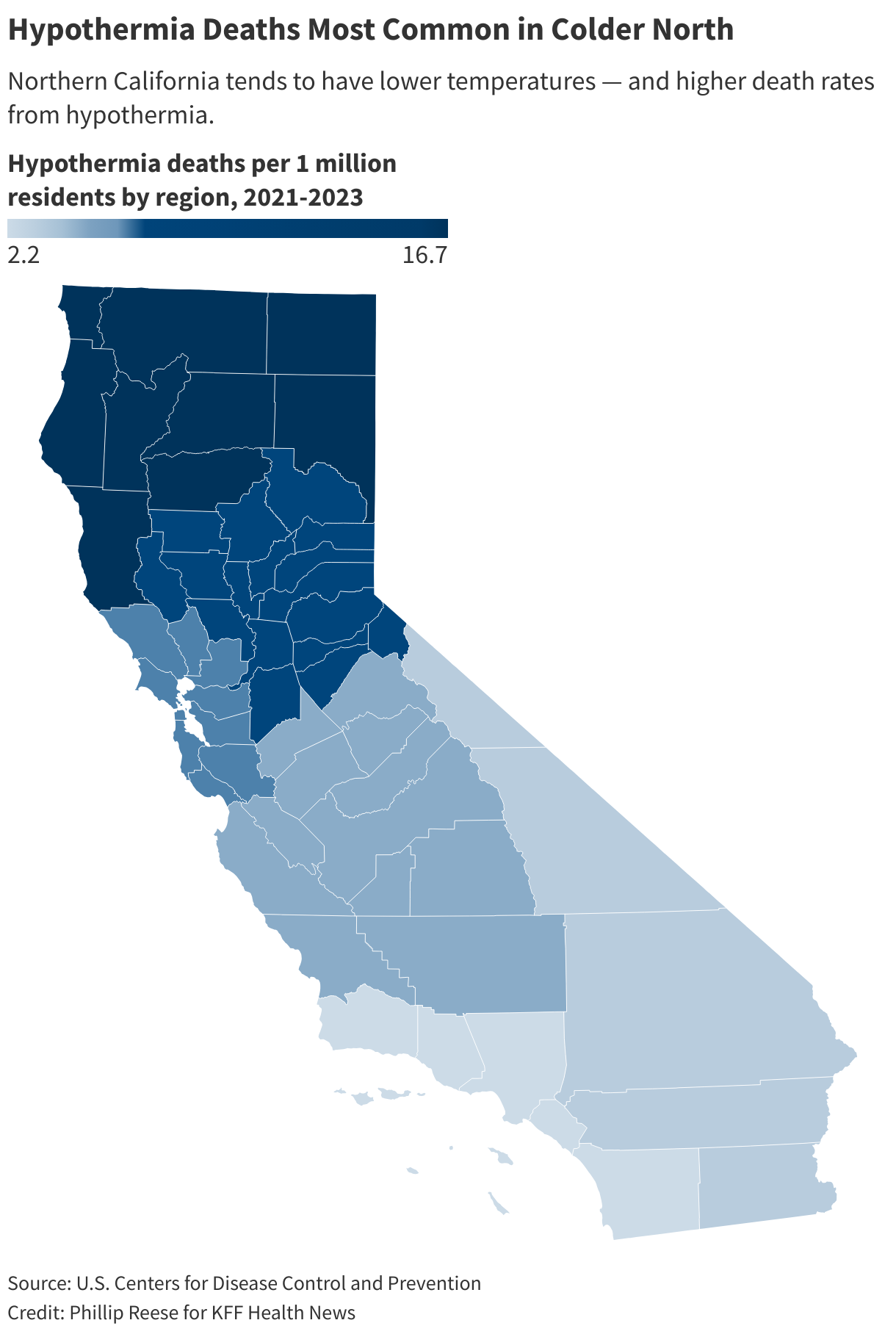
California’s hypothermia death rate is highest in its rural, mountainous, northern counties, but most deaths are occuring in urban centers.
Hypothermia was the underlying or contributing cause of death for 46 Los Angeles County residents from 2021 to 2023 — the highest number in the state. However, the death rate was below the statewide average due to the county’s large population.
Santa Clara, San Francisco, and Sacramento had the highest hypothermia death rates among the state’s most populous counties. Hypothermia was the underlying or a contributing cause of 42 deaths in Santa Clara County from 2021 through 2023, up from 11 during the previous three years, CDC data shows.
“Every year, we are worse than last year,” said Shaunn Cartwright, an advocate for homeless people in Santa Clara County.
Cartwright said local officials are not providing enough permanent shelter beds for homeless people, let alone enough temporary shelter beds on cold nights. It’s a problem that Kushel said is prevalent across the state.
Michelle Jorden, Santa Clara County’s chief medical examiner, said in an emailed statement that she is unsure why hypothermia deaths are rising but is monitoring the trend. She said the county has sent outreach teams to encampments with supplies, , and issued cold weather safety alerts during severe conditions.
Sacramento County had 34 deaths related to hypothermia from 2021 through 2023, up from 20 hypothermia deaths from 2018 through 2020. Like many places, Sacramento has enforced homeless ordinances and in the wake of a U.S. Supreme Court decision giving cities more authority to fine and remove homeless people from the streets. Nearly half of unsheltered homeless Californians report that officials have confiscated their belongings at some point, Kushel said.
Bob Erlenbusch, an advocate at the , said many homeless people are cold because local authorities have confiscated items including blankets, sleeping bags, and tents during sweeps.
“They’re not supposed to take people’s stuff,” he said. “They’re supposed to tag it and store it, but that doesn’t happen.”
City of Sacramento spokesperson Jennifer Singer said city workers reach out to homeless residents before removing encampments “so they can manage their belongings before any clean-up begins.”
Kushel said the long-term solution to the rise in hypothermia deaths is to prevent people from falling into homelessness and get those who are already homeless into housing. In the meantime, she said, cities need to open more warming centers — and cooling centers in the summer — and make sure they are accessible.
This article was produced by Ńîąóĺú´«Ă˝Ň•îl Health News, which publishes , an editorially independent service of the .
Ńîąóĺú´«Ă˝Ň•îl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/rural-health/california-freezing-deaths-increase-older-people-homeless/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1958235&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>She thought little of it at first. She did routine self-checks and kept up with medical appointments. But a relative urged her to get a mammogram. She took the advice and learned she had stage 3 breast cancer, a revelation that stunned her.
“I’m 36 years old, right?” said Kashiwada, a civil engineer in Sacramento, California. “No one’s thinking about cancer.”
About 11,000 Asian American and Pacific Islander women were diagnosed with breast cancer in 2021 and about 1,500 died. The latest federal data shows the rate of new breast cancer diagnoses in Asian American and Pacific Islander women — a group that once had relatively low rates of diagnosis — is rising much faster than that of many other racial and ethnic groups. The trend is especially sharp among young women such as Kashiwada.
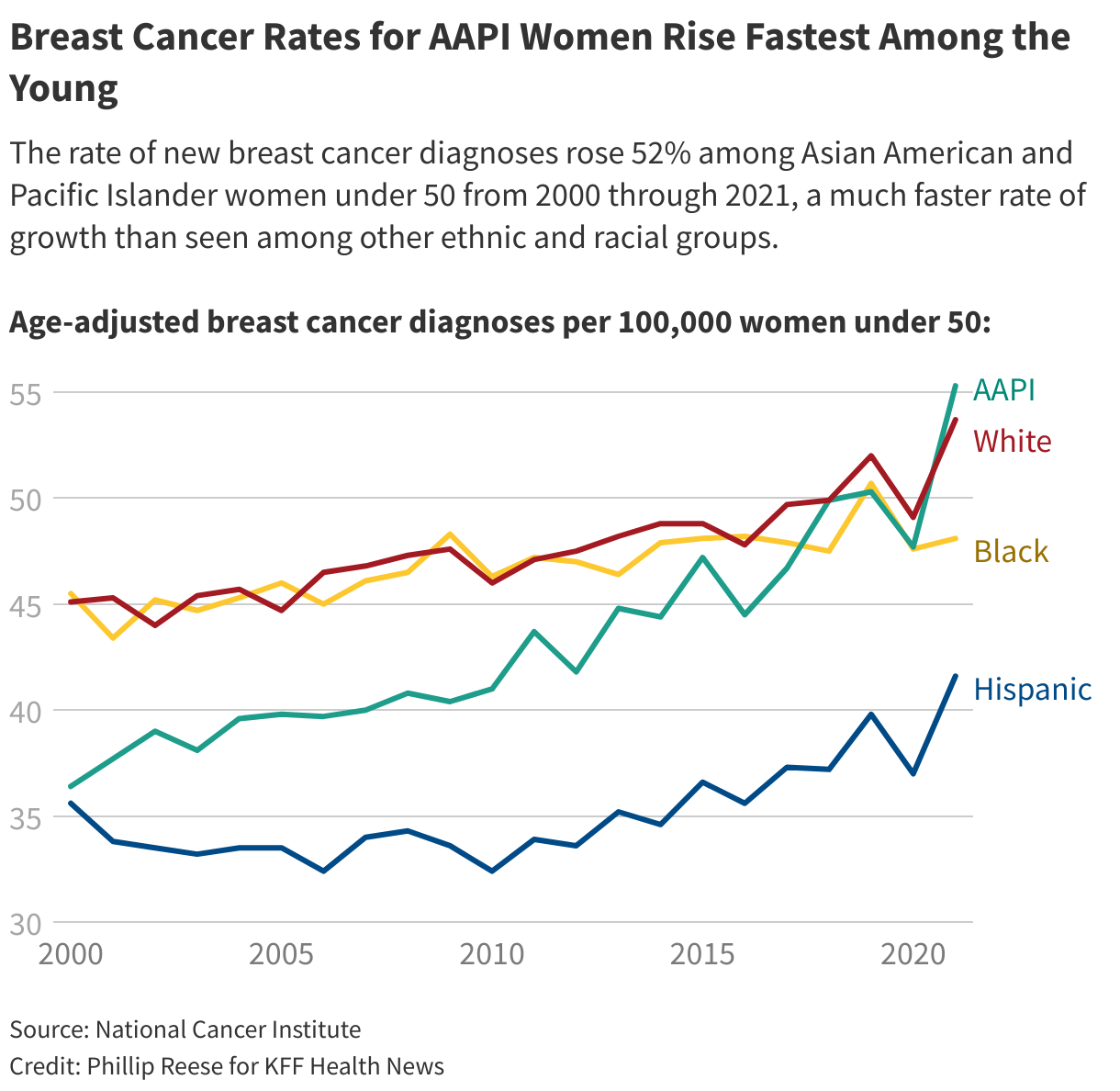
About 55 of every 100,000 Asian American and Pacific Islander women under 50 were diagnosed with breast cancer in 2021, surpassing the rate for Black and Hispanic women and on par with the rate for white women, according to from the National Institutes of Health. (Hispanic people can be of any race or combination of races but are grouped separately in this data.)
The rate of new breast cancer cases among Asian American and Pacific Islander women under 50 grew by about 52% from 2000 through 2021. Rates for AAPI women 50 to 64 grew 33% and rates for AAPI women 65 and older grew by 43% during that period. By comparison, the rate for women of all ages, races, and ethnicities grew by 3%.
Researchers have picked up on this trend and are racing to find out why it is occuring within this ethnically diverse group. They suspect the answer is complex, ranging from cultural shifts to pressure-filled lifestyles — yet they concede it remains a mystery and difficult for patients and their families to discuss because of cultural differences.
, director of the Clinical Breast Cancer Program at UC Davis Health, said the Asian American diaspora is so that simple explanations for the increase in breast cancer aren’t obvious.
“It’s a real trend,” Chew said, adding that “it is just difficult to tease out exactly why it is. Is it because we’re seeing an influx of people who have less access to care? Is it because of many things culturally where they may not want to come in if they see something on their breast?”
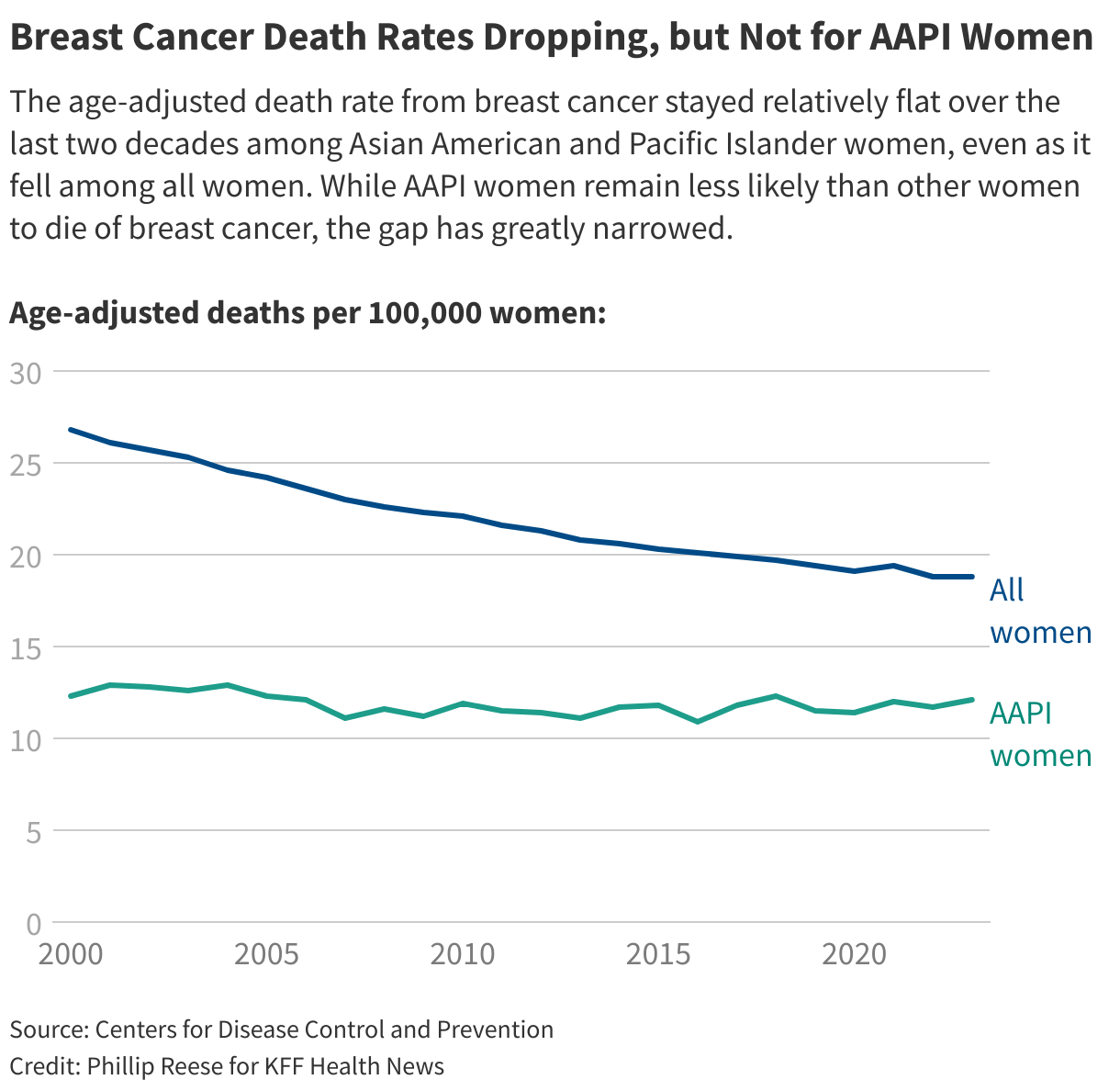
There’s urgency to solve this mystery because it’s costing lives. While women in most ethnic and racial groups are experiencing sharp declines in breast cancer death rates, about Asian American and Pacific Islander women of any age died from breast cancer in 2023, essentially the same death rate as in 2000, according to age-adjusted, provisional data from the Centers for Disease Control and Prevention. The breast cancer death rate among all women during that period dropped 30%.
The CDC does not break out breast cancer death rates for many different groups of Asian American women, such as those of Chinese or Korean descent. It has, though, begun distinguishing between Asian American women and Pacific Islander women.
Nearly 9,000 Asian American women died from breast cancer from 2018 through 2023, compared with about 500 Native Hawaiian and Pacific Islander women. However, breast cancer death rates were among Native Hawaiian and Pacific Islander women than among Asian American women during that period.
Rates of , , , and cancer, along with rates, have also recently risen significantly among Asian American and Pacific Islander women under 50, NIH data show. Yet breast cancer is much more common among young AAPI women than any of those other types of cancer — especially concerning because young women are more aggressive forms of the disease, with high mortality rates.
“We’re seeing somewhere almost around a 4% per-year increase,” said , a professor and epidemiologist at the University of California-San Francisco’s Helen Diller Family Comprehensive Cancer Center. “We’re seeing even more than the 4% per-year increase in Asian/Pacific Islander women less than age 50.”
Gomez is a lead investigator on a exploring the causes of cancer in Asian Americans. She said there is not yet enough research to know what is causing the recent spike in breast cancer. The answer may involve multiple risk factors over a long period of time.
“One of the hypotheses that we’re exploring there is the role of stress,” she said. “We’re asking all sorts of questions about different sources of stress, different coping styles throughout the lifetime.”
It’s likely not just that there’s more screening. “We looked at trends by stage at diagnosis and we are seeing similar rates of increase across all stages of disease,” Gomez said.
, a professor and epidemiologist at the Keck School of Medicine of the University of Southern California, said the trend may be related to Asian immigrants adopting some lifestyles that put them at higher risk. Setiawan is a breast cancer survivor who was diagnosed a few years ago at the age of 49.
“Asian women, American women, they become more westernized so they have their puberty younger now — having earlier age at [the first menstrual cycle] is ,” said Setiawan, who is working with Gomez on the cancer study. “Maybe , we delay childbearing, — those are all associated with breast cancer risks.”
, a professor at the University of California-Davis and an , added that only of NIH funding is devoted to researching cancer among Asian Americans.
Whatever its cause, the trend has created years of anguish for many patients.
Kashiwada underwent a mastectomy following her breast cancer diagnosis. During surgery, doctors at UC Davis Health discovered the cancer had spread to lymph nodes in her underarm. She underwent eight rounds of chemotherapy and 20 sessions of radiation treatment.
Throughout her treatments, Kashiwada kept her ordeal a secret from her grandmother, who had helped raise her. Her grandmother never knew about the diagnosis. “I didn’t want her to worry about me or add stress to her,” Kashiwada said. “She just would probably never sleep if she knew that was happening. It was very important to me to protect her.”
Kashiwada moved in with her parents. Her mom took a leave from work to help take care of her.
Kashiwada’s two young children, who were 3 and 6 at the time, stayed with their dad so she could focus on her recovery.
“The kids would come over after school,” she said. “My dad would pick them up and bring them over to see me almost every day while their dad was at work.”
Kashiwada spent months regaining strength after the radiation treatments. She returned to work but with a doctor’s instruction to avoid lifting heavy objects.
Kashiwada had her final reconstructive surgery a few weeks before covid lockdowns began in 2020. But her treatment was not finished.
Her doctors had told her that estrogen fed her cancer, so they gave her medicine to put her through early menopause. The treatment was not as effective as they had hoped. Her doctor performed surgery in 2021 to remove her ovaries.
More recently, she was diagnosed with osteopenia and will start injections to stop bone loss.
Kashiwada said she has moved past many of the negative emotions she felt about her illness and wants other young women, including Asian American women like her, to be aware of their elevated risk.
“No matter how healthy you think you are, or you’re exercising, or whatever you’re doing, eating well, which is all the things I was doing — I would say it does not make you invincible or immune,” she said. “Not to say that you should be afraid of everything, but just be very in tune with your body and what your body’s telling you.”

Phillip Reese is a data reporting specialist and an associate professor of journalism at California State University-Sacramento.
This article was produced by Ńîąóĺú´«Ă˝Ň•îl Health News, which publishes , an editorially independent service of the . Supplemental support comes from the through .
Ńîąóĺú´«Ă˝Ň•îl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/race-and-health/breast-cancer-rates-increase-asian-american-pacific-islander-women/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1903134&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>On New Year’s Day 2022, at age 31, Hermida learned he had HIV.
“I thought I was going to die,” he said, recalling how a chill washed over him as he reviewed his results. He struggled to navigate a new, convoluted health care system. Through an HIV organization he found online, he received a list of medical providers to call in Washington, D.C., where he was at the time, but they didn’t return his calls for weeks. Hermida, who speaks only Spanish, didn’t know where to turn.
By the time of Hermida’s diagnosis, the U.S. Department of Health and Human Services was about three years into a to end the nation’s HIV epidemic by pumping hundreds of millions of dollars annually into certain states, counties, and U.S. territories with the highest infection rates. The goal was to reach the estimated people living with HIV, including some who don’t know they have the disease.
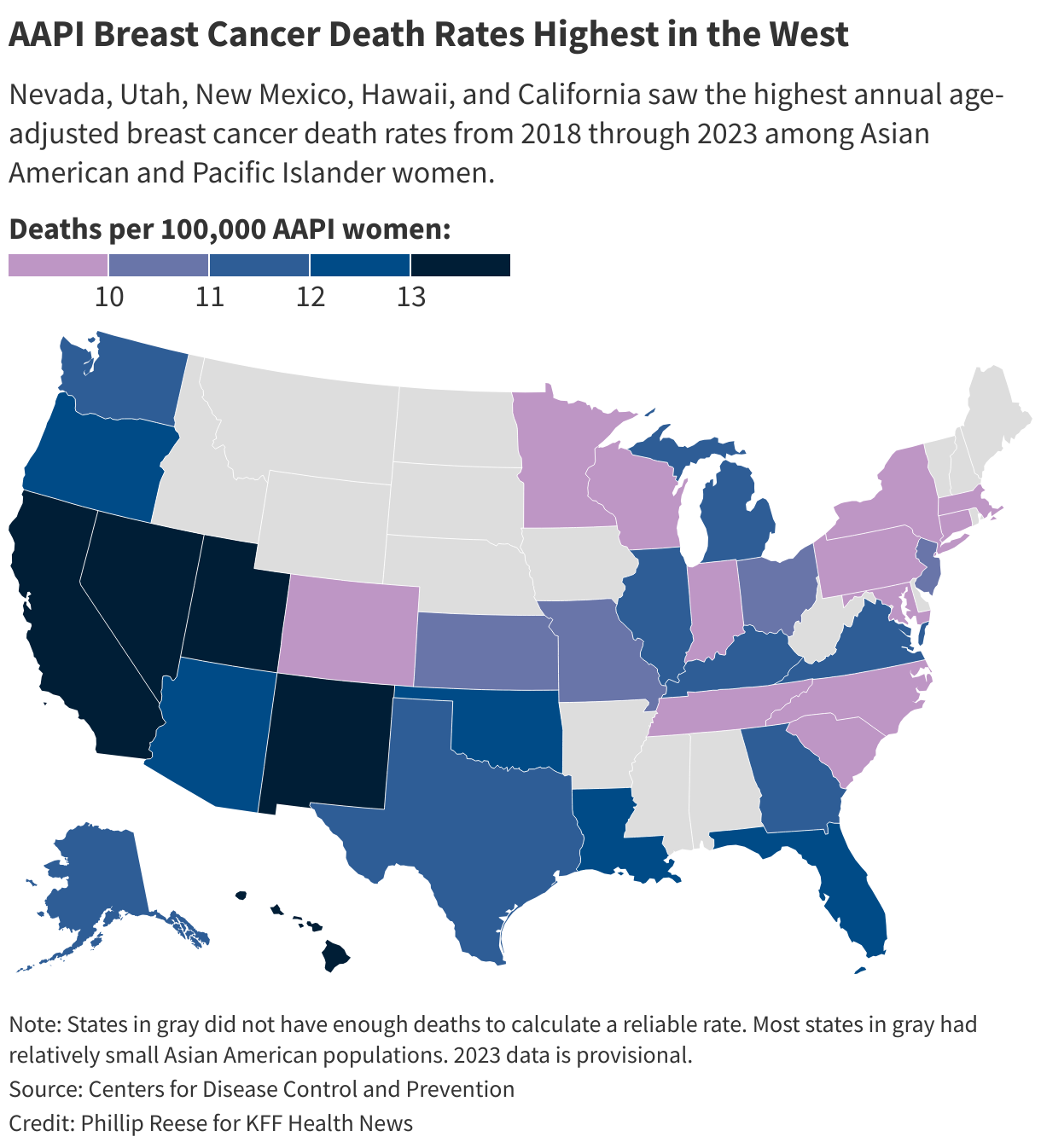
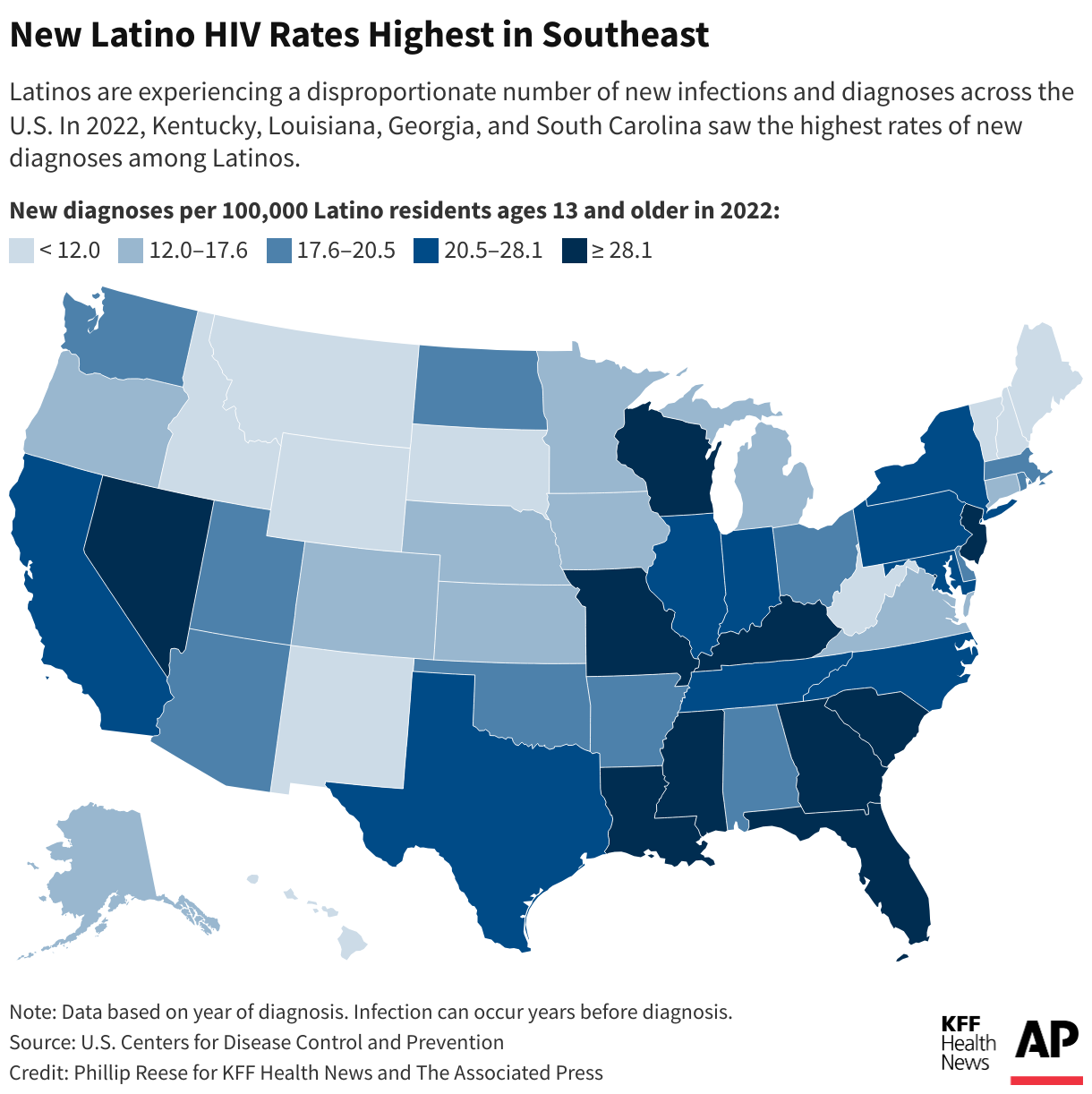
Overall, estimated new HIV infection rates declined 23% from 2012 to 2022. But a Ńîąóĺú´«Ă˝Ň•îl Health News-Associated Press analysis found the rate has not fallen for Latinos as much as it has for other racial and ethnic groups.
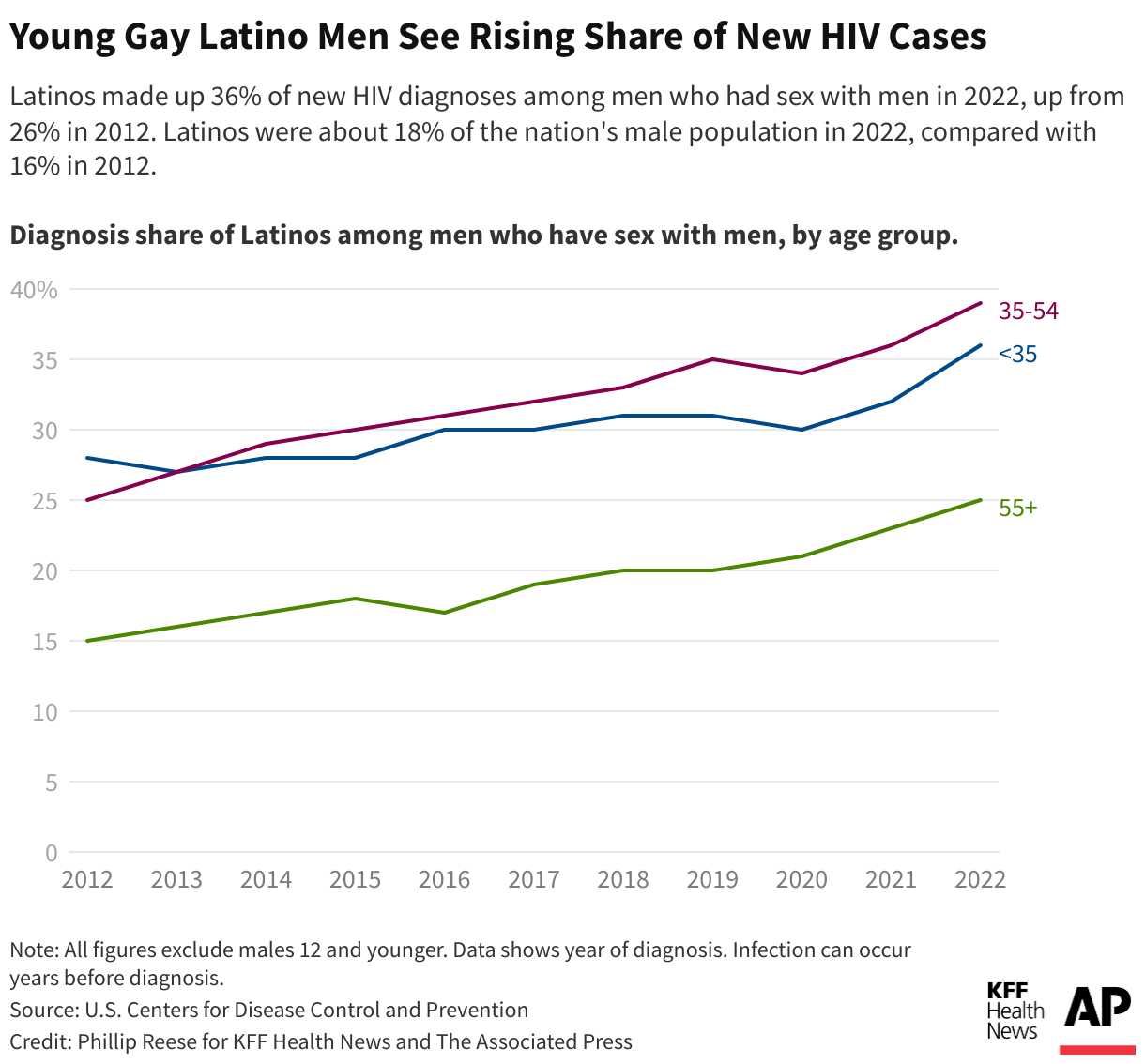
While African Americans continue to have the highest HIV rates in the United States overall, Latinos made up the largest share of new HIV diagnoses and infections among gay and bisexual men in 2022, per the most recent data available, compared with other racial and ethnic groups. Latinos, who make up about 19% of the U.S. population, accounted for about 33% of new HIV infections, according to the Centers for Disease Control and Prevention.
The analysis found Latinos are experiencing a disproportionate number of new infections and diagnoses across the U.S., with diagnosis rates highest in the Southeast. Public health officials in Mecklenburg County, North Carolina, and Shelby County, Tennessee, where data shows diagnosis rates have gone up among Latinos, told Ńîąóĺú´«Ă˝Ň•îl Health News and the AP that they either don’t have specific plans to address HIV in this population or that plans are still in the works. Even in well-resourced places like San Francisco, California, HIV diagnosis rates grew among Latinos in the last few years while falling among other racial and ethnic groups despite the county’s goals to reduce infections among Latinos.
“HIV disparities are not inevitable,” Robyn Neblett Fanfair, director of the CDC’s Division of HIV Prevention, said in a statement. She noted the systemic, cultural, and economic inequities — such as racism, language differences, and medical mistrust.
And though the CDC provides some funds for minority groups, Latino health policy advocates want HHS to declare a public health emergency in hopes of directing more money to Latino communities, saying current efforts aren’t enough.
“Our invisibility is no longer tolerable,” said Vincent Guilamo-Ramos, of the Presidential Advisory Council on HIV/AIDS.
Lost Without an Interpreter
Hermida suspects he contracted the virus while he was in an open relationship with a male partner before he came to the U.S. In late January 2022, months after his symptoms started, he went to a clinic in New York City that a friend had helped him find to finally get treatment for HIV.
Too sick to care for himself alone, Hermida eventually moved to Charlotte, North Carolina, to be closer to family and in hopes of receiving more consistent health care. He enrolled in an clinic that receives funding from the Ryan White HIV/AIDS Program, a federal safety-net plan that serves over half of those in the nation diagnosed with HIV, regardless of their citizenship status.
His HIV became undetectable after he was connected with case managers. But over time, communication with the clinic grew less frequent, he said, and he didn’t get regular interpretation help during visits with his English-speaking doctor. An Amity Medical Group representative confirmed Hermida was a client but didn’t answer questions about his experience at the clinic.
Hermida said he had a hard time filling out paperwork to stay enrolled in the Ryan White program, and when his eligibility expired in September 2023, he couldn’t get his medication.
He left the clinic and enrolled in a health plan through the Affordable Care Act marketplace. But Hermida didn’t realize the insurer required him to pay for a share of his HIV treatment.


In January, the Lyft driver received a $1,275 bill for his antiretroviral — the equivalent of 120 rides, he said. He paid the bill with a coupon he found online. In April, he got a second bill he couldn’t afford.
For two weeks, he stopped taking the medication that keeps the virus undetectable and intransmissible.
“Estoy que colapso,” he said. I’m falling apart. “Tengo que vivir para pagar la medicación.” I have to live to pay for my medication.
One way to prevent HIV is preexposure prophylaxis, or PrEP, which is regularly taken to reduce the risk of getting HIV through sex or intravenous drug use. It was in 2012 but the uptake has not been even across racial and ethnic groups: CDC data show much lower rates of PrEP coverage among Latinos than among white Americans.
Epidemiologists say high PrEP use and consistent access to treatment are necessary to build community-level resistance.
Carlos Saldana, an infectious disease specialist and former medical adviser for Georgia’s health department, five clusters of rapid HIV transmission involving about 40 gay Latinos and men who have sex with men from February 2021 to June 2022. Many people in the cluster told researchers they had not taken PrEP and struggled to understand the health care system.
They experienced other barriers, too, Saldana said, including lack of transportation and fear of deportation if they sought treatment.
Latino health policy advocates want the federal government to redistribute funding for HIV prevention, including testing and access to PrEP. Of the in federal money that went toward things like HIV health care services, treatment, and prevention in 2022, only 4% went to prevention, .
They suggest more money could help reach Latino communities through efforts like faith-based outreach at churches, testing at clubs on Latin nights, and training bilingual HIV testers.

Latino Rates Going Up
Congress has appropriated over five years to the Ending the HIV Epidemic initiative, and jurisdictions that get the money are of it in community-based organizations. But the initiative lacks requirements to target any particular groups, including Latinos, leaving it up to the cities, counties, and states to come up with specific strategies.
In 34 of the 57 areas getting the money, cases are going the wrong way: Diagnosis rates among Latinos increased from 2019 to 2022 while declining for other racial and ethnic groups, the Ńîąóĺú´«Ă˝Ň•îl Health News-AP analysis found.
Starting Aug. 1, state and local health departments will have to provide annual spending reports on funding in places that account for 30% or more of HIV diagnoses, the CDC said. Previously, it had been required for only a small number of states.
In some states and counties, initiative funding has not been enough to cover the needs of Latinos.
South Carolina, which saw rates nearly double for Latinos from 2012 to 2022, hasn’t expanded HIV mobile testing in rural areas, where the need is high among Latinos, said Tony Price, HIV program manager in the state health department. South Carolina can pay for only four community health workers focused on HIV outreach — and not all of them are bilingual.
In Shelby County, Tennessee, home to Memphis, the Latino HIV diagnosis rate rose 86% from 2012 to 2022. The health department said it got $2 million in initiative funding in 2023 and while the acknowledges that Latinos are a target group, department director Michelle Taylor said: “There are no specific campaigns just among Latino people.”
Up to now, Mecklenburg County, North Carolina, didn’t include specific targets to address HIV in the Latino population — where rates of new diagnoses more than doubled in a decade but fell slightly among other racial and ethnic groups. The health department has used funding for bilingual marketing campaigns and awareness about PrEP.
Moving for Medicine
When it was time to pack up and move to Hermida’s third city in two years, his fiancé, who is taking PrEP, suggested seeking care in Orlando, Florida.
The couple, who were friends in high school in Venezuela, had some family and friends in Florida, and they had heard about Pineapple Healthcare, a nonprofit primary care clinic dedicated to supporting Latinos living with HIV.
The clinic is housed in a medical office south of downtown Orlando. Inside, the mostly Latino staff is dressed in pineapple-print turquoise shirts, and Spanish, not English, is most commonly heard in appointment rooms and hallways.
“At the core of it, if the organization is not led by and for people of color, then we’re just an afterthought,” said , the community outreach director at Pineapple Healthcare, who was diagnosed with HIV in 2013.



“¿Te mudaste reciente, ya por fin?” asked nurse practitioner Eliza Otero. Did you finally move? She started treating Hermida while he still lived in Charlotte. “Hace un mes que no nos vemos.” It’s been a month since we last saw each other.
They still need to work on lowering his cholesterol and blood pressure, she told him. Though his viral load remains high, Otero said it should improve with regular, consistent care.
Pineapple Healthcare, which doesn’t receive initiative money, offers full-scope primary care to mostly Latino males. Hermida gets his HIV medication at no cost there because the clinic is part of a federal drug discount program.
The clinic is in many ways an oasis. The new diagnosis rate for Latinos in Orange County, Florida, which includes Orlando, rose by about a third from 2012 through 2022, while dropping by a third for others. Florida has the third-largest Latino population in the U.S., and had the seventh-highest rate of new HIV diagnoses among Latinos in the nation in 2022.
Hermida, whose asylum case is pending, never imagined getting medication would be so difficult, he said during the 500-mile drive from North Carolina to Florida. After hotel rooms, jobs lost, and family goodbyes, he is hopeful his search for consistent HIV treatment — which has come to define his life the past two years — can finally come to an end.
“Soy un nómada a la fuerza, pero bueno, como me comenta mi prometido y mis familiares, yo tengo que estar donde me den buenos servicios médicos,” he said. I’m forced to be a nomad, but like my family and my fiancé say, I have to be where I can get good medical services.
That’s the priority, he said. “Esa es la prioridad ahora.”

Ńîąóĺú´«Ă˝Ň•îl Health News and The Associated Press analyzed data from the U.S. Centers for Disease Control and Prevention on the number of new HIV diagnoses and infections among Americans ages 13 and older at the local, state, and national levels. This story primarily uses incidence rate data — estimates of new infections — at the national level and diagnosis rate data at the state and county level.
Bose reported from Orlando, Florida. Reese reported from Sacramento, California. AP video journalist Laura Bargfeld contributed to this report.
The Associated Press Health and Science Department receives support from the Robert Wood Johnson Foundation. The AP is responsible for all content.
This article was produced by Ńîąóĺú´«Ă˝Ň•îl Health News, which publishes , an editorially independent service of the .
A Project of Ńîąóĺú´«Ă˝Ň•îl Health News and The Associated Press
Co-Published by Univision Noticias
CREDITS
Reporters:
Vanessa G. Sánchez
Devna Bose
Phillip Reese
Cinematography:
Laura Bargfeld
Photography:
Laura Bargfeld
Phelan M. Ebenhack
Video Editing:
Federica Narancio
Kathy Young
Esther Poveda
Additional Video:
Federica Narancio
Esther Poveda
Web Production:
Eric Harkleroad
Lydia Zuraw
Special thanks to
Lindsey Dawson
Editors:
Judy Lin
Erica Hunzinger
Data Editor:
Holly Hacker
Social Media:
Patricia Vélez
Federica Narancio
Esther Poveda
Carolina Astuya
Natalia Bravo
Juan Pablo Vargas
Kyle Viterbo
Sophia Eppolito
Hannah Norman
Chaseedaw Giles
Tarena Lofton
Translation:
Paula Andalo
Copy Editing:
Gabe Brison-Trezise
This <a target="_blank" href="/public-health/young-gay-latinos-increase-hiv-diagnosis-incidence/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1871562&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>