The care was ordinary. A hospital in Modesto, California, treated a 30-year-old man for shoulder and back pain after a car accident. He went home in less than three hours.
The bill was extraordinary. Sutter Health Memorial Medical Center charged $44,914 including an $8,928 ŌĆ£trauma alertŌĆØ fee, billed for summoning the hospitalŌĆÖs top surgical specialists and usually associated with the most severely injured patients.
The case, buried in the records of a 2017 trial, is a rare example of a courtroom challenge to something billing consultants say is increasingly common at U.S. hospitals.
Tens of thousands of times a year, hospitals charge enormously expensive trauma alert fees for injuries so minor the patient is never admitted.
In Florida alone, where the number of trauma centers has exploded, hospitals charged such fees more than 13,000 times in 2019 even though the patient went home the same day, according to a KHN analysis of state data provided by Etienne Pracht, an economist at the University of South Florida. Those cases accounted for more than a quarter of all the stateŌĆÖs trauma team activations that year and were more than double the number of similar cases in 2014, according to an all-payer database of hospital claims kept by FloridaŌĆÖs Agency for Health Care Administration.
While false alarms are to be expected, such frequent charges for little if any treatment suggest some hospitals see the alerts as much as a money spigot as a clinical emergency tool, claims consultants say.
ŌĆ£Some hospitals are using it as a revenue generator,ŌĆØ Tami Rockholt, a registered nurse and medical claims consultant who appeared as an expert witness in the Sutter Health car-accident trial, said in an interview. ŌĆ£ItŌĆÖs being taken advantage ofŌĆØ and such cases are ŌĆ£way more numerousŌĆØ than a few years ago, she said.
Hospitals can charge trauma activation fees when a crack squad of doctors and nurses assembles after an ambulance crew says itŌĆÖs approaching with a patient who needs trauma care. The idea is that life-threatening injuries need immediate attention and that designated trauma centers should be able to recoup the cost of having a team ready ŌĆö even if it never swings into action.
Those fees, which can exceed $50,000 per patient, are billed on top of what hospitals charge for emergency medical care.
ŌĆ£We do see quite a bit of non-appropriate trauma charges ŌĆö more than youŌĆÖd see five years ago,ŌĆØ said Pat Palmer, co-founder of Beacon Healthcare Costs Illuminated, which analyzes thousands of bills for insurers and patients. Recently ŌĆ£we saw a trauma activation fee where the patient walked into the ERŌĆØ and walked out soon afterward, she said.
The portion of Florida trauma activation cases without an admission rose from 22% in 2012 to 27% last year, according to the data. At one Florida facility, Broward Health Medical Center, there were 1,285 trauma activation cases in 2019 with no admission ŌĆö almost equal to the number that led to admissions.
ŌĆ£Trauma alerts are activated by EMS [first responders with emergency medical services], not hospitals, and we respond accordingly when EMS activates a trauma alert from the field,ŌĆØ said Jennifer Smith, a Broward Health spokesperson.
Florida regulations allow hospitals themselves to declare an ŌĆ£in-hospital trauma alertŌĆØ for ŌĆ£patients not identified as a trauma alertŌĆØ in the field, according to by the Florida Department of Health.
At some hospitals, few patients whose cases generate trauma alerts are treated and released the same day.
At Regions Hospital, a Level I trauma center in St. Paul, Minnesota, patients who are not admitted after a trauma team alert are ŌĆ£very rareŌĆØ ŌĆö 42 of 828 cases last year, or about 5%, said Dr. Michael McGonigal, the centerŌĆÖs director, who blogs at ŌĆ£.ŌĆØ
ŌĆ£If youŌĆÖre charging an activation fee for all these people who go home, ultimately thatŌĆÖs going to be a red flagŌĆØ for Medicare and insurers, he said.
In the Sutter case in Modesto, the patient sued a driver who struck his vehicle, seeking damages from the driver and her insurer. Patient ŌĆ£looks good,ŌĆØ an emergency doctor wrote in the records, which were part of the trial evidence. He prescribed Tylenol with hydrocodone for pain.
ŌĆ£If someone is not going to bleed out, or their heart is not going to stop, or theyŌĆÖre not going to quit breathing in the next 30 minutes, they probably do not need a trauma team,ŌĆØ Rockholt said in her testimony.
Like other California hospitals with trauma center designations, Sutter Health Memorial Medical Center follows ŌĆ£county-designated criteriaŌĆØ for calling an activation, said Sutter spokesperson Liz Madison: ŌĆ£The goal is to remain in position to address trauma cases at all times ŌĆö even in the events where a patient is determined healthy enough to be treated and released on the same day.ŌĆØ
Trauma centers regularly review and revise their rules for trauma team activation, said Dr. Martin Schreiber, trauma chief at Oregon Health & Science University and board chair at the Trauma Center Association of America, an industry group.
ŌĆ£It is not my impression that trauma centers are using activations to make money,ŌĆØ he said. ŌĆ£Activating patients unnecessarily is not considered acceptable in the trauma community.ŌĆØ
Hospitals began billing trauma team fees to insurers of all kinds after Medicare authorized them for cases in which hospitals are notified of severe injuries before a patient arrives. Instead of leaving trauma team alerts to the paramedics, hospitals often call trauma activations themselves based on information from the field, trauma surgeons say.
Reimbursement for trauma activations is complicated. Insurers donŌĆÖt always pay a hospitalŌĆÖs trauma fee. Under rules established by Medicare and a committee of insurers and health care providers, emergency departments must give 30 minutes of critical care after a trauma alert to be paid for activating the team. For inpatients, the trauma team fee is sometimes folded into other charges, billing consultants say.
But, on the whole, the increase in the size and frequency of trauma team activation fees, including those for non-admitted patients, has helped turn trauma operations, often formerly a financial drain, into profit centers. In recent years, hundreds of hospitals have sought trauma center designation, which is necessary to bill a trauma activation fee.
ŌĆ£There must have been a consultant that ran around the country and said, ŌĆśHey hospitals, why donŌĆÖt you start charging this, because you can,ŌĆÖŌĆØ said Marc Chapman, founder of , which challenges large hospital bills for auto insurers and other payers. ŌĆ£In many of those cases, the patients are never admitted.ŌĆØ
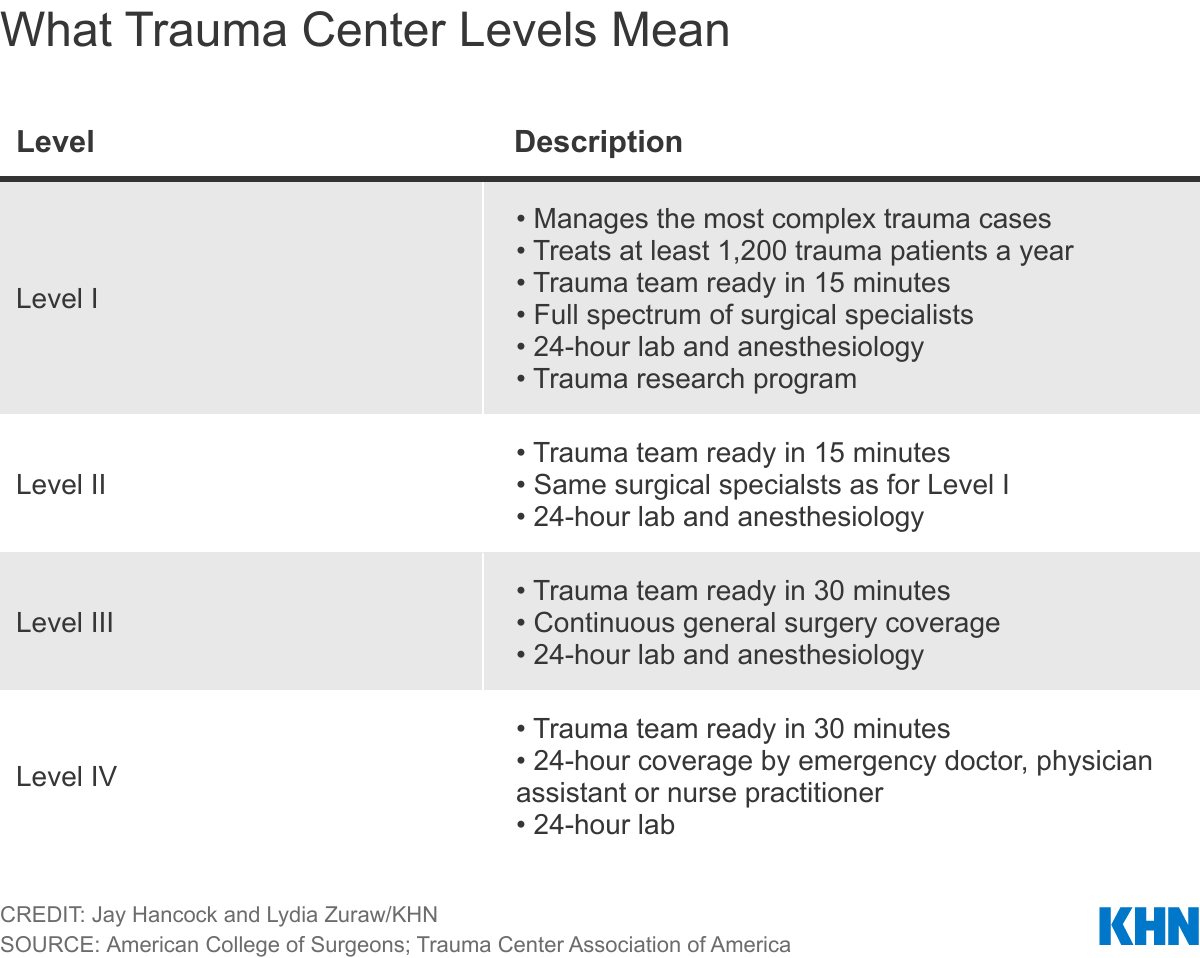
The national number of Level I and Level II trauma centers, able to treat the most badly hurt patients, grew from 305 in 2008 to 567 last year, according to the American College of Surgeons. Hundreds of other hospitals have Level III or Level IV trauma centers, which can treat less severe injuries and also bill for trauma team activation, although often at lower rates.
Emergency surgeons say they walk a narrow path between being too cautious and activating a team unnecessarily (known as ŌĆ£overtriageŌĆØ) and endangering patients by failing to call a team when severe injuries are not obvious.
Often ŌĆ£we donŌĆÖt know if patients are seriously injured in the field,ŌĆØ said Dr. Craig Newgard, a professor of emergency medicine at Oregon Health & Science University. ŌĆ£The EMS providers are using the best information they have.ŌĆØ
Too many badly hurt patients still donŌĆÖt get the care they need from trauma centers and teams, Newgard argues.
ŌĆ£WeŌĆÖre trying to do the greatest good for the greatest number of people from a system perspective, recognizing that itŌĆÖs basically impossible to get triage right every time,ŌĆØ he said. ŌĆ£YouŌĆÖre going to take some patients to major trauma centers who donŌĆÖt really end up having serious injury. And itŌĆÖs going to be a bit more expensive. But the trade-off is optimizing survival.ŌĆØ
At Oregon Health & Science, 24% of patients treated under trauma alerts over 12 months ending this spring were not admitted, Schreiber said.
ŌĆ£If this number gets much lower, you could put patients who need activation at risk if they are not activated,ŌĆØ he said.
On the other hand, rising numbers of trauma centers and fees boost health care costs. The charges are passed on through higher insurance premiums and expenses paid not just by health insurers but also auto insurers, who often are first in line to pay for the care of a crash victim.
Audits are uncommon and often the system is geared to paying claims with little or no scrutiny, billing specialists say. Legal challenges like the one in the Sutter case are extremely rare.
ŌĆ£Most of these insurers, especially auto insurance, do not look at the bill,ŌĆØ said Beth Morgan, CEO of Medical Bill Detectives, a consulting firm that helps insurers challenge hospital charges. ŌĆ£They automatically pay it.ŌĆØ
And trauma activation charges also can hit patients directly.
ŌĆ£Sometimes the insurance companies will not pay for them. So people could get stuck with that bill,ŌĆØ Morgan said.
A few years ago, Zuckerberg San Francisco General Hospital charged a $15,666 trauma response fee to the family of a toddler who had fallen off a hotel bed. He was fine. Treatment was a bottle of formula and a nap. The hospital waived the fee after KHN and Vox wrote about it.
Trauma alert fatigue can add up to a nonfinancial cost for the trauma team itself, McGonigal said.
ŌĆ£Every time that pager goes off, youŌĆÖre peeling a lot of people away from their jobs only to see [patients] go home an hour or two later,ŌĆØ he said.
ŌĆ£Some trauma centers are running into problems because they run themselves ragged. And there is probably unneeded expense in all the resources that are needed to evaluate and manage those patients.ŌĆØ
čŅ╣¾Õ·┤½├ĮęĢŅl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFFŌĆöan independent source of health policy research, polling, and journalism. Learn more about .